- | Healthcare Healthcare
- | Expert Commentary Expert Commentary
- |
Projected Medicaid Expansion Costs Just Rose Again
Earlier this month the Centers for Medicare and Medicaid Services (CMS) actuary published a score of the House bill to repeal and replace the Affordable Care Act (ACA). Contained within that score is a concerning update of CMS’s projections for the costs of the ACA’s Medicaid expansion. Incredibly, the latest projections now indicate that per capita expansion costs will remain more than 50% higher, through 2022, than previously projected.
When the ACA first passed it was expected that the per capita cost of covering its Medicaid expansion population (childless adults under the age of 65 up to 138% of the federal poverty line) would be substantially less than for the adults under 65 who were already on Medicaid. This seemed a perfectly sensible prediction. After all, the already-eligible population included individuals (such as pregnant women) with substantial known health care needs. Accordingly, as seen in Figure 1, the 2013 Medicaid actuarial report projected that the cost of covering newly eligible adults would be $3,625 per person in 2016. This was substantially lower than the same report’s projection of 2016 per capita costs of $5,002 for covering previously eligible adults. 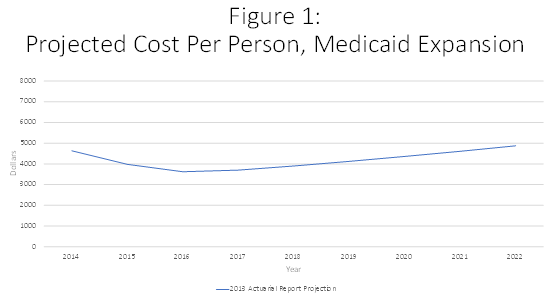
These early projections, however, failed to anticipate the substantial cost growth that would arise from states under the ACA being able to pass 100% of expansion costs on to the federal government. Figure 2 shows that in both 2015 and 2016 per-capita Medicaid expansion costs came in more than 60% higher than the earlier projections, as reflected in the 2016 actuarial report. 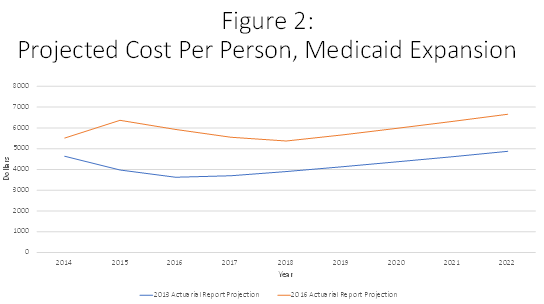
The 2016 Medicaid actuarial report noted that states had attributed the high initial expansion costs to “pent-up demand,” as well as to states having anticipated that “the persons who were most likely to enroll in the first year would be those with the greatest health care needs.” Accordingly, CMS projected that the unexpected initial cost surge would soon ebb, gradually lowering per-capita costs through 2018. Thereafter per-capita costs would rise only gradually such that through 2021 they would still be below the heights they had climbed to in 2015. In support of this projection, CMS offered the hopeful take that “the effects of pent-up demand and adverse selection are expected to end after the earliest years of the eligibility expansion, and more recent information . . . indicates that the average costs of newly eligible adults were significantly lower than the States anticipated.”
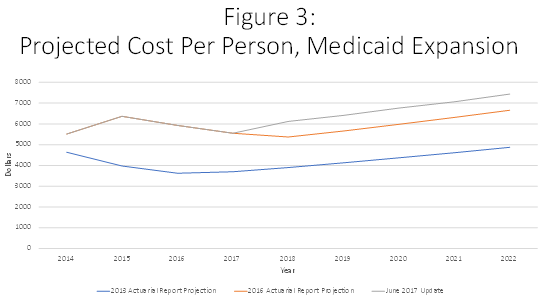
What this all means is that CMS now expects that through 2022, Medicaid expansion costs will be $7,436 per person, more than 50% higher than the $4,875 projected in the 2013 report. Thus, rather than just being an initial burst due to pent-up demand, this excess cost is now seen as a permanent feature of the ACA’s Medicaid expansion.
The latest CMS projections show other concerning trends as well. From 2018 to 2026, per capita expenditures for covering the expansion population are now projected to grow more rapidly than they are for Medicaid’s more vulnerable historically eligible population of pregnant women, poor children, seniors and disabled. This rapid expansion expenditure growth would occur on top of the unexpectedly large costs in evidence to date. In other words, expansion has made Medicaid spending more poorly targeted. We’re already spending a far greater share than expected on Medicaid’s relatively less needy participants, and this poor targeting is expected to grow worse.
Lawmakers are currently debating whether and how to modify the ACA’s substantial expansion of Medicaid. CMS’s latest projections show the per capita costs of that expansion rising still further beyond prior expectations.