- | Healthcare Healthcare
- | Expert Commentary Expert Commentary
- |
After Healthcare, Americans Still Have Plenty to Spend
The notion that healthcare spending is bankrupting Americans is false
The United States spends more on healthcare than any other country—in the aggregate, per capita, and as a percentage of gross domestic product (GDP). This generates a lot of hand-wringing, reflected in headlines: “Health care costs are bankrupting us.” “The real reason health care is bankrupting America.” “Health care will bankrupt the nation.”
Part of this concern is the perception that healthcare spending critically reduces our capacity to purchase things other than healthcare. As one writer put it, “[M]andatory health spending is increasingly crowding out spending in areas that would also otherwise enhance economic output and productivity, such as education and infrastructure.”
Is healthcare, in fact, dangerously crimping our ability to spend money on other things—food, housing, transportation, education, leisure goods, etc.? International data offers some hints. While there are other ways to analyze the question, simple metrics suggest that, compared with residents of other wealthy countries, Americans still have ample spending power for non-healthcare-related goods and services.
These metrics don’t tell us whether the level of US healthcare spending is optimal, whether the quality of US care matches up with the quality in other countries, or whether costs stress the budgets of particular populations (e.g., the uninsured) or institutions (e.g., state governments). They also don’t tell us how our non-healthcare spending will look 20 or 30 years from now.
What the numbers do show is that despite our high level of healthcare spending, Americans have more money for non-healthcare goods and services than almost any other people in the world.
Graham’s blogpost: US versus Canada
In 2016, John Graham, a Canadian economist who has worked both in Canada and the US (including as a contributor to the Mercatus Center), wondered about these questions and ran some simple, but illuminating numbers. In a blogpost for Canada’s Fraser Institute, Graham found that “although US health-care spending is very inefficient, there is little evidence that it subtracts from spending on other goods and services.” Table 1 shows his numbers, along with percentage calculations based on those numbers: 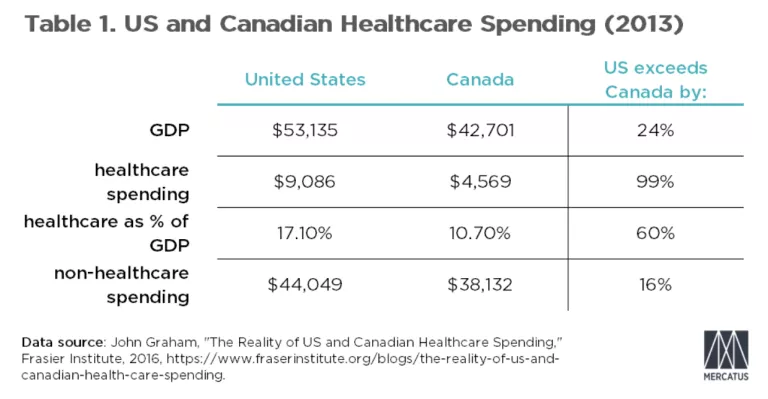
Our numbers: US versus OECD
The analysis can be extended to the 37 members of the Organisation for Economic Co-operation and Development (OECD)—the club of developed countries.

Table 2 reveals several things: At $9,236, the United States’ healthcare spending is the world’s highest by far. According to these numbers, the United States spends 88 percent more per capita than Australia, the second-ranking nation in this category. As a percentage of GDP, US healthcare spending is 48 percent higher than second-place Belgium—15.5 percent versus 10.4 percent.
Among these countries, the United States ranks 3rd in per capita GDP. Luxembourg’s GDP is around 51 percent higher than the United States’, while Ireland’s is around 8 percent higher. And in 4th and 5th places, Norway’s per capita GDP is around 3 percent lower than the United States’, and Australia’s is around 13 percent lower.
However, the United States’ outsize healthcare spending barely alters its non-healthcare rankings. After healthcare spending, the United States drops from 3rd to 4th in terms of spending on things other than healthcare. Rather than being 2 percent behind Americans, Norwegians end up with 5 percent more than Americans to spend on things other than healthcare. But Americans still have more money to spend on non-healthcare goods and services than the other 24 countries in the chart do.
This raises a fundamental question: if healthcare spending is not a crisis in Canada or elsewhere in the OECD, by what logical standard is it a crisis in the United States, where average Americans still have considerably more to spend on non-healthcare goods? That’s a real question to ponder—not a rhetorical exercise.
Should we and can we spend less on healthcare?
Again, none of this means the United States’ level of healthcare spending is efficient. There’s a widespread perception that the United States spends more than it ought to on medical services and that this situation is reversible. There are, however, reasons to doubt this perception.
First, exactly why the United States spends so much is a matter of dispute. A widely cited study co-authored by the late Uwe Reinhardt finds that Americans spend more because healthcare prices are higher.
The anonymous (but highly knowledgeable) blogger Random Critical Analysis (RCA) rejects this analysis, arguing that statistics indicate that it is the volume of healthcare consumed, not the prices, that drives higher US spending. In an impressive statistical display, RCA also argues that healthcare-to-GDP is an inappropriate standard by which to judge healthcare spending. Rather, RCA argues, it’s more meaningful to compare healthcare spending to “actual individual consumption” (AIC).
AIC represents public and private expenditures on goods and services consumed individually, as opposed to those consumed collectively (like roads and defense). By this criterion, the United States is close to the norm for developed countries because AIC occupies a considerably larger share of the US economy than the European Union (EU) economy (in part because of lower US savings). In other words, the ratio of spending on healthcare (which is mostly controlled by individuals) to total spending by individuals is similar in America to the ratios in other countries. RCA’s analysis mirrors similar arguments made here, here, and here.
Others (including our Mercatus colleague Alex Tabarrok and his co-author Eric Helland) argue that the costs of US healthcare are high because the resources demanded in healthcare (especially high-skilled labor) are also in high and well-compensated demand in other sectors. US physicians, for example, are paid more than their counterparts in Canada and many other OECD countries because the sort of person who becomes a doctor could as easily attract high compensation in other fields in America—and less so in the other countries.
John Graham writes, “When an American physician laments the state of medicine, and encourages her child to become a computer scientist or investment banker instead, this is what she is talking about. So, it’s highly unlikely that we could reduce U.S. physicians’ incomes, and maintain an adequate supply of them, without destroying the opportunity for Americans (and immigrants) to earn high incomes in lots of different fields.”
Software engineer and blogger Peter Laakmann argues (persuasively, we think) that high US healthcare costs stem largely from factors outside of healthcare—high incomes, high accumulated wealth, and low rates of saving. He believes reforming US healthcare will not alter these macroeconomic fundamentals.
The flip side of this spending-too-much argument is the getting-too-little argument. There are plenty of legitimate concerns about US healthcare. Perhaps the quality of care is in some ways wanting, compared with other countries, though that too is a dubious proposition. California State University at Northridge economist Glen Whitman and Stanford University neurologist Scott Atlas have both argued that the most widely cited study ranking countries by the quality of their health systems—the World Health Organization’s (WHO) World Health Report—is profoundly flawed.
WHO, they argued, arbitrarily built its health-system rankings in ways that would purposely skew the results against the United States. Among other problems, the WHO writers accepted without question dubious data provided by other governments and manufactured other data via questionable methodologies. They implicitly assumed that all variation in health in different countries is explained by those countries’ healthcare systems (when these systems likely explain only around 10 percent of such variation). Furthermore, they arbitrarily imposed the authors’ preferences regarding tax policy and income distribution as indicators of healthcare system quality. In other words, Whitman and Atlas argue, the WHO indexes mostly measure things other than “How well does this country’s healthcare system improve its population’s health?”
Healthcare isn’t bankrupting us
Perhaps Americans spend too much on healthcare, though that truism is more debatable than public discourse would suggest. Perhaps, for all they spend on healthcare, Americans are not getting their money’s worth—though that argument may be overblown, as well. And perhaps healthcare spending is not such a big problem today but will be in the future. At least for now, the data suggests that unlike in all but a few countries, heavy-duty spending on healthcare still leaves Americans with plenty of money to buy other things.
Cecilia Bellet is an economic fellow at the US Consumer Product Safety Commission.
Photo by PixelsEffect