- | Healthcare Healthcare
- | Expert Commentary Expert Commentary
- |
What is Virtual Health?: The Promise of Technology and the Chaos of Terminology
Virtual health is arguably the most important contemporary development in American healthcare. Remote communication and intelligent machines are poised to revolutionize the capabilities and outreach of healthcare providers. However, the terminology surrounding these technologies is chaotic, with broad disagreement over what is meant by “virtual health,” “telehealth,” “telemedicine,” and “autonomous health.” These terms are often used interchangeably and inconsistently, complicating research and confusing policy discussions at a critical juncture. Our goal is to provide some historical context to virtual health and more clearly define the terminology.
Long before the pandemic, physicians and other healthcare providers were interacting with patients via electronic devices. The earliest type of “remote care” was conducted by telegraph. Then, the telephone’s appearance in 1876 vastly increased the frequency of remote patient/provider interactions. Thirty years later, a doctor transmitted an electrocardiogram report from a lab to a hospital one mile away by telephone; in 1948, clinicians sent radiology reports 24 miles by phone; in 1959, University of Nebraska clinicians used two-way television to transmit neurological exams to medical students on campus; and five years later, the Nebraska team conducted video consultations and speech-therapy sessions with patients in a hospital 112 miles away.
In 1967, Massachusetts General Hospital used television cameras to establish a remote clinic inside Boston’s Logan Airport to serve distressed passengers. In recent decades, telehealth has even been used to conduct surgery and diagnose cancer in Antarctica and to manage an astronaut’s blood clot on the International Space Station. In the past two decades, Skype, FaceTime and other apps enabled laypersons to engage in interactive video communication.
Yet, despite the promise of virtual health, it remained a mere niche in the healthcare industry until COVID-19 emerged. In a year when social distancing became a lifesaving imperative, we saw a vast increase in healthcare at a distance. With patients, providers, payers, and regulators now fully acclimated to the service, virtual health will almost certainly remain a widely used component of healthcare long after the pandemic subsides.
Given that virtual health is likely here to stay, it would be helpful for the terminology to be consistent. For a glimpse of the problem, consider these three views of how virtual health has been defined in recent years:
- An Aetna International webpage suggests that virtual health is a synonym for video-based telehealth. “Virtual care is the capability to access a doctor through a video call on your phone or computer, anytime, anywhere in the world.”
- The Care Innovations consulting group describes virtual health as a narrower concept than telehealth, writing, “Virtual healthcare is actually a component of telehealth, which is a broader term encompassing the entirety of remote and/or technology-driven healthcare.”
- PriceWaterhouse Canada views virtual health as closer to what we imagine—a concept broader than mere telehealth: “Virtual health … includes health-care professionals who collect patient data and deliver care remotely, giving patients and caregivers more transparency (i.e., full visibility of their care plans, clinical histories, authorizations and more) and influence in how, when and where they’re treated. And virtual health goes beyond interactions with physicians, such as visits with chiropractors and therapists as well as interactions with pharmacists and insurance providers. It also includes an abundance of health and wellness apps and mobile monitoring devices.”
The Taxonomy of Virtual Health
Berkowitz, Ommen, and Halamka summarized all healthcare in one simple graphic. All care is either on-site (the patient and the provider are face-to-face) or virtual (patient and provider are in separate locations). Telehealth involves direct communication between patient and provider. Autonomous health involves interactions between a patient and a computer system, or between a provider and a computer system. Autonomous health can include the application of expert systems, artificial intelligence, and machine learning to support diagnosis, treatment, and compliance monitoring. These intelligent machines can be used to educate, monitor, advise, or treat patients.
Building on that diagram, in Figure 1, we add details. In place of “office visit,” we have “non-hospital visit,” which may occur in a provider’s office, the patient’s home or workplace, or elsewhere.
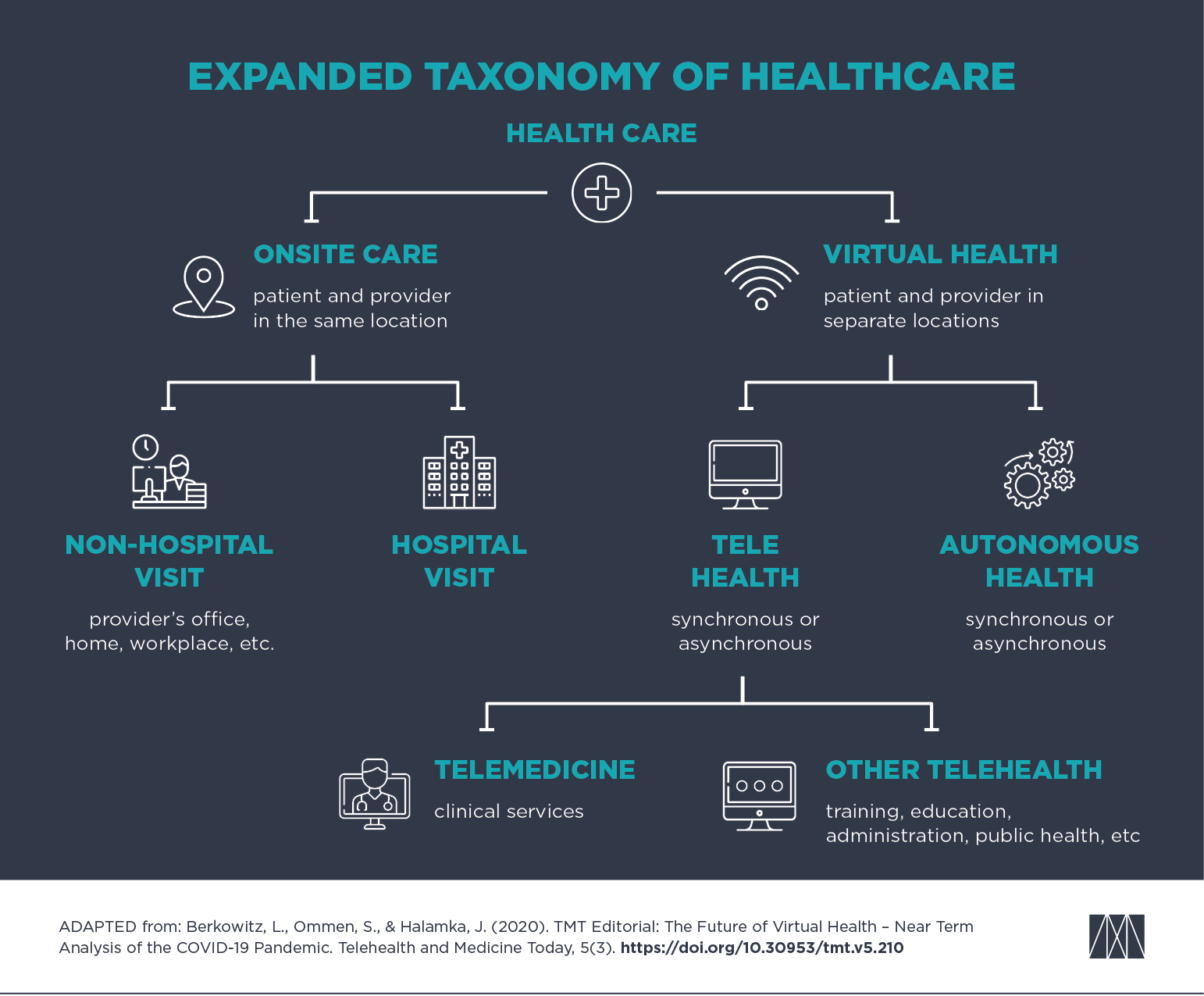
Figure 1: Taxonomy of Healthcare
The federal government’s Health Resources and Services Administration defines telehealth as “[t]he use of electronic information and telecommunications technologies to support and promote long-distance clinical health care, patient and professional health-related education, public health and health administration.”
The Center for Connected Health Policy identifies four distinct ways of delivering telehealth: video conferencing (two-way interaction); store and forward (“transmission of digital images, pictures, video, or text”); remote patient monitoring (“transmission of health or medical data”); and mobile health, or mHealth (“the use of mobile devices such as tablets and smartphones to transmit health information”).
“Telehealth” and “telemedicine” are not synonyms. Rather, telemedicine comprises a portion of telehealth. The American Academy of Family Physicians makes the distinction: “While telemedicine refers specifically to remote clinical services, telehealth can refer to remote non-clinical services such as provider training, continuing medical education or public health education, administrative meetings and electronic information sharing to facilitate and support assessment, diagnosis, consultation, treatment, education, and care management.”
In a telemedicine visit, the federal government’s Medicaid website refers to the provider’s location as the “distant site” or “hub site” and the patient’s location as the “originating site” or “spoke site.”
Next, Figure 2 further details the types of virtual health, separating both telehealth and autonomous health into synchronous and asynchronous components. Our definitions are aimed at describing the technology—not the law. For example, a telephone call between patient and provider is clearly an example of telehealth, but some jurisdictions or payors exclude audio-only telephone calls from their definition of telehealth, and do not reimburse them.
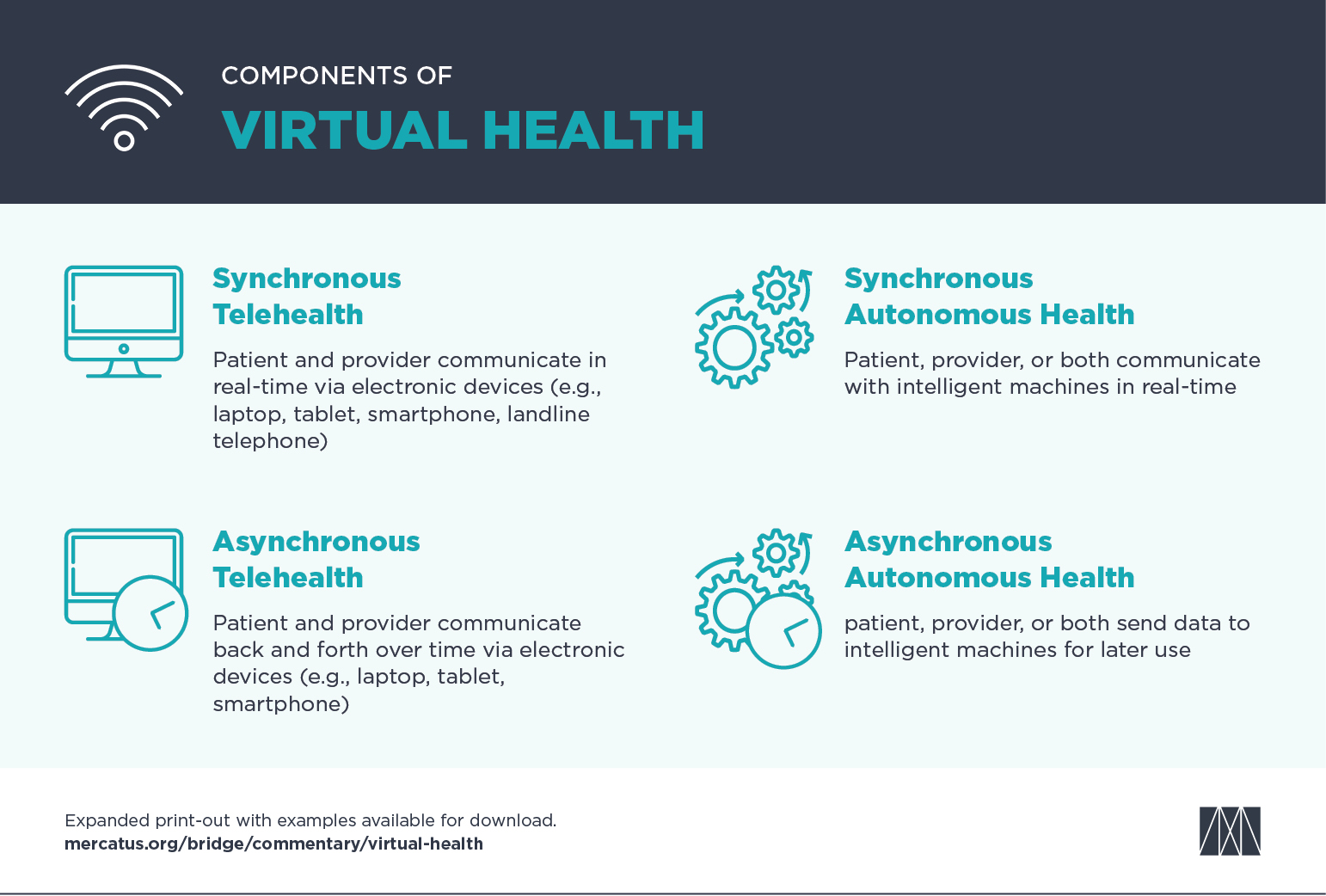
Figure 2: Components of Virtual Health
Conclusion
It is commonly stated that America faces a coming physician shortage. But as one co-author (Berkowitz) said, “the answer may not be in increasing the number of professionals available, but in using them more efficiently in a team-based fashion.” He also described how better use of automation, virtualization, and delegation would let a primary care physician and their team care for a much larger population more efficiently. Another co-author (Graboyes) argued that a more efficient, cost-effective healthcare system would come from “shifting some tasks from the physician’s calendar to non-physicians (like nurses or technicians), intelligent machines (like computer diagnostics), or patients themselves (by using home diagnostic equipment, for example). Digital technologies make this possible in previously unimaginable ways.”
These changes are not implying something is unnecessary or in need of replacement. Rather, as Modern Healthcare argued, “Virtual health is not about technology replacing humans in health care, but about augmenting and supplementing providers to improve the delivery of care—moving from a focus on bedside to ‘webside’ manner. Virtual care may help relieve clinicians of mundane, administrative, or routine tasks, affording them more opportunities to practice at the top of their license.”
As evident, the current terminology of virtual health is jumbled and inconsistent. Having a shared language so that a dialogue about the way to move forward can truly progress across clinical, research, regulatory, reimbursement, and other public health arenas would be helpful. By suggesting this set of pragmatic definitions, it is our hope that individuals making critical decisions about virtual health will benefit from a standard framework.
Finally, the terms “synchronous telehealth,” “asynchronous telehealth,” “synchronous autonomous health,” and “asynchronous autonomous health” might sound a tad abstract. So, Figure 3 shows real-world examples of each of these four categories.
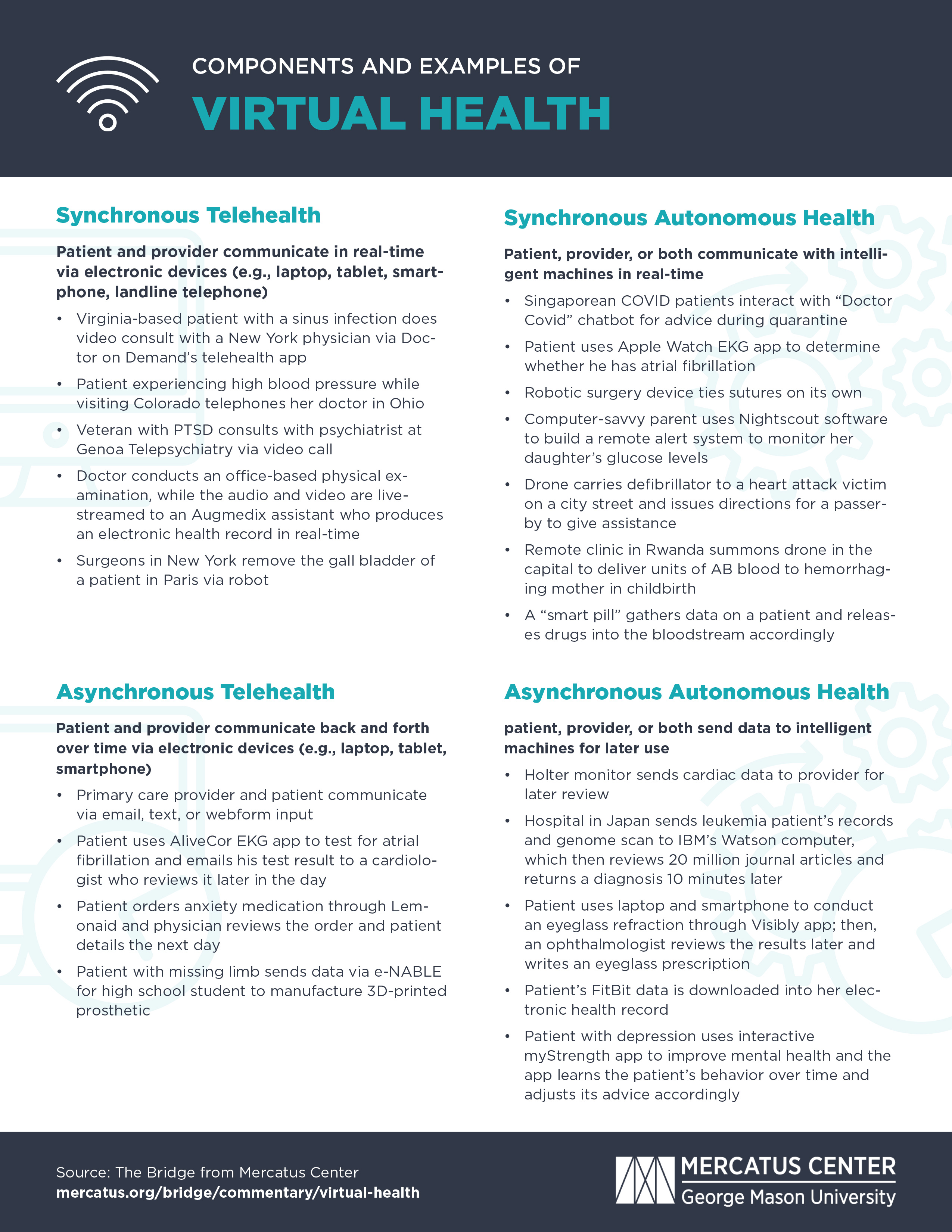
Figure 3: Components and Examples of Virtual Health