- | Healthcare Healthcare
- | Feature Feature
- |
Certificate-of-Need Laws: How They Affect Healthcare Access, Quality, and Cost
What years of study reveals about the effectiveness of CON programs
Certificate-of-need (CON) laws require healthcare providers to seek permission from state regulators before they offer new services, expand facilities, or invest in technology. While the original hope was that CON laws would restrain healthcare costs, increase healthcare quality, and improve access to care for poor and underserved communities, a large body of academic research suggests that CON laws have instead limited access, degraded quality, and increased cost.
Despite this poor track record, CON laws remain in 35 states and the District of Columbia, keeping millions of Americans from getting the care they need.
Given the evidence from academic research and the experience of states which have undertaken reform, state policymakers who wish to increase patient access to high-quality, lower-cost care would be well advised to eliminate their entire CON programs. Reforming CON laws also represents a valuable step policymakers can take to improve the responsiveness of their healthcare systems in times of crisis. See below for research related to CON laws and the COVID-19 pandemic.
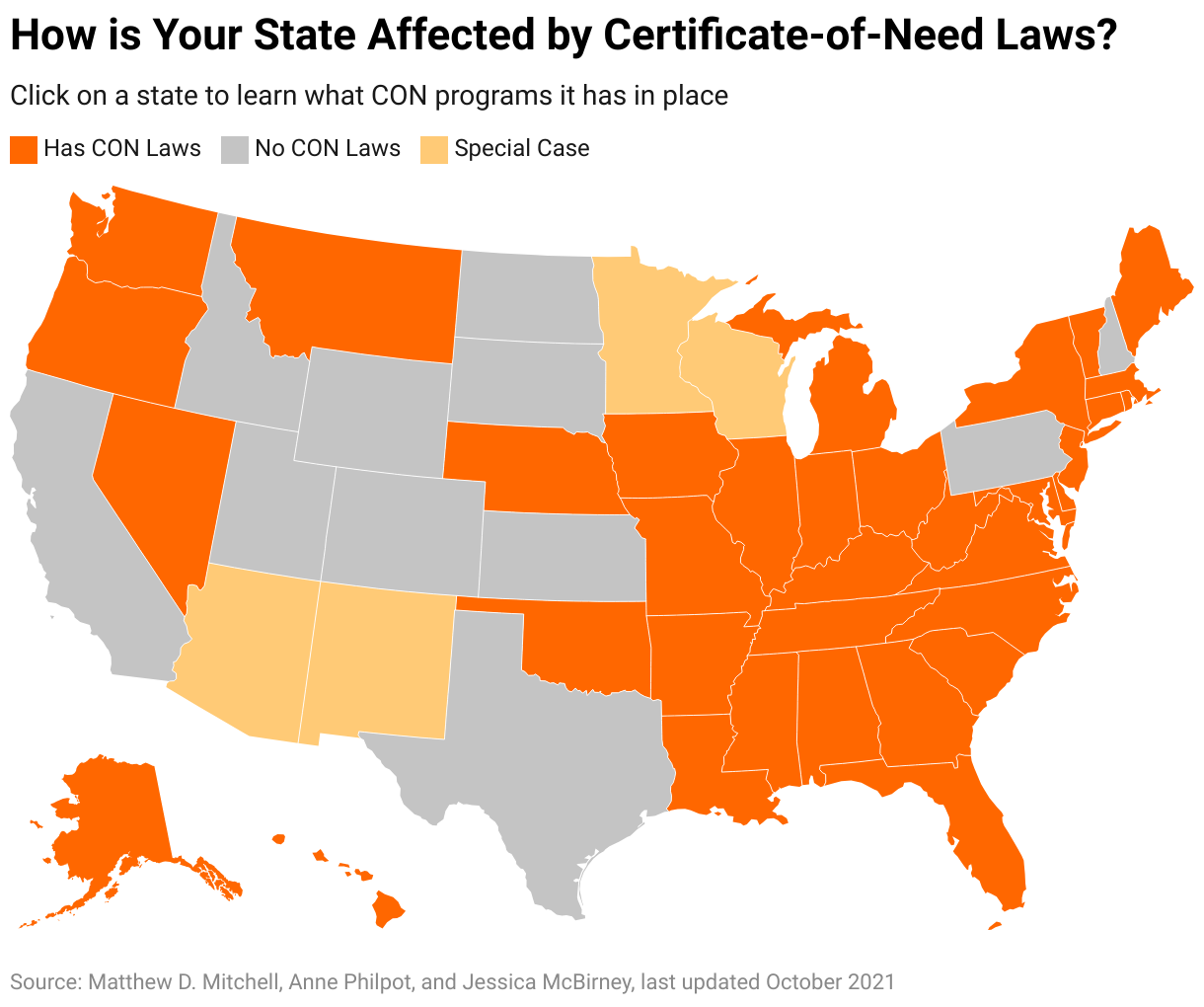
Which States Have Certificate-of-Need Laws?
As of May 2021, 35 states and the District of Columbia required providers to obtain a CON before offering at least one healthcare service. Two additional states, Minnesota and Wisconsin, set numerical caps on certain services such as the total number of hospital beds and nursing home beds. Other states require a CON for ground and air aPeoplembulance services, though these laws are often found in transportation statutes, and their effects on health outcomes are not as well studied. Hawaii has the highest number of CON restrictions (28) of any state, with North Carolina (27) and the District of Columbia (25) following close behind. Eleven states have removed all CON laws or caps: California, Colorado, Idaho, Kansas, New Hampshire, North Dakota, Pennsylvania, South Dakota, Texas, Utah, and Wyoming.
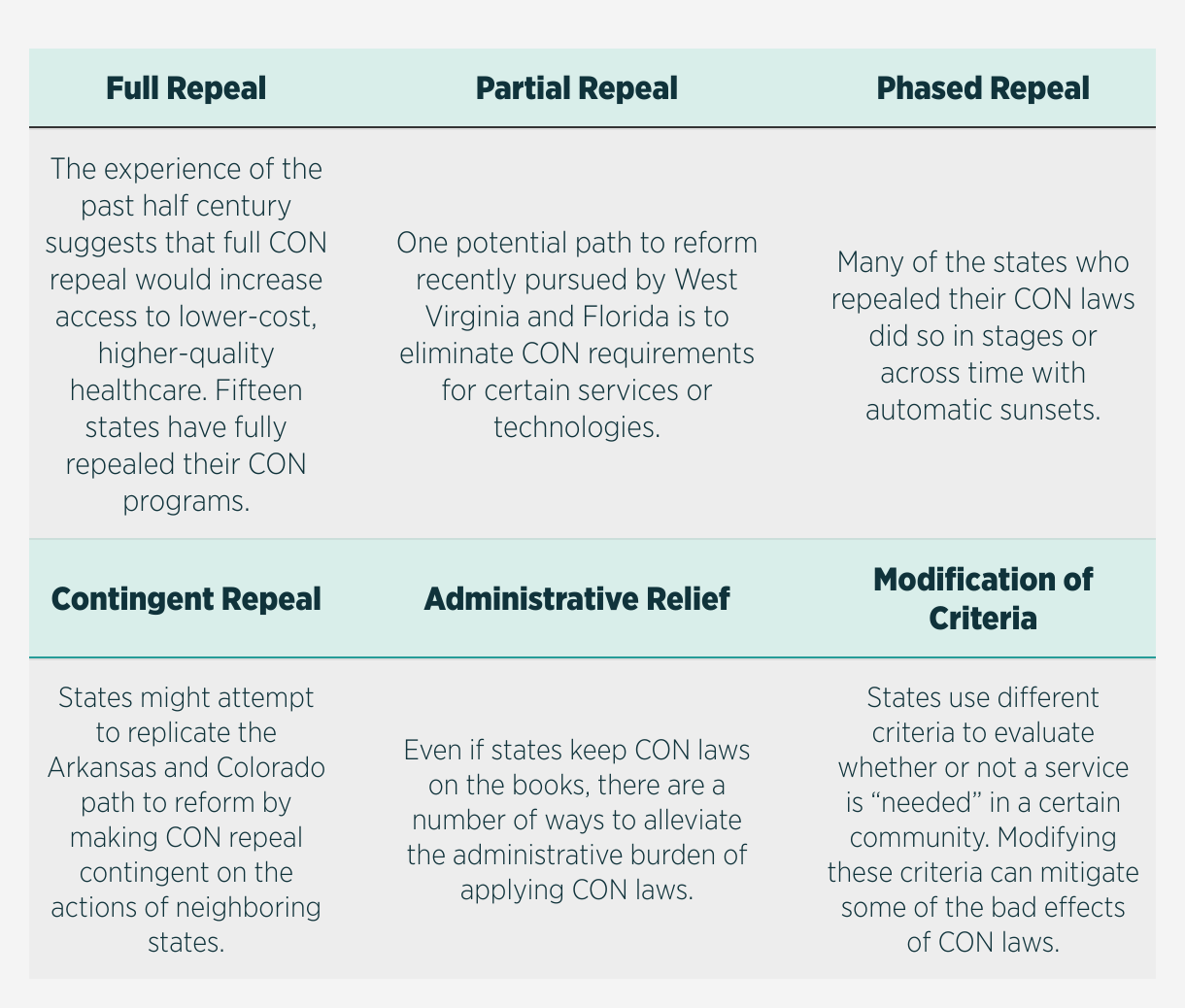
Options For Reforming Certificate-of-Need Laws
Many legislators see CON repeal as a common-sense way of improving healthcare in their states. While research shows full repeal is best, there are still ways to make meaningful reform happen even when full repeal is not feasible. Click on one of the reform options below to learn more about it.
If you'd like to schedule a consultation with one of our scholars on CON reform, email our outreach team.
More on Certificate-Of-Need Laws
Click on a topic below to learn more about CON laws. You can also visit our 2020 update on the state of CON laws across the country.
New York was the first state to institute a CON program in 1964, followed by Rhode Island, Maryland, California, and 22 other states over the next 10 years. In 1974, Congress passed the National Health Planning and Resources Development Act, requiring states to implement CON requirements in order to receive funding through certain federal programs. Louisiana was the only state not to implement a CON program during this time. But in 1986—as evidence mounteed that CON laws were failing to control healthcare costs or improve quality or access—the federal government repealed the CON mandate, and many states immediately began retiring their CON programs. Since then, 15 states have done away with their CON regulations. A majority of states still maintain CON programs, however, and vestiges of the National Health Planning and Resources Development Act can be seen in the justifications that state legislatures offer in support of these regulations, despite evidence they are ineffective. Learn more about how CON laws have changed over the past several decades.
No. CON regulation explicitly limits the establishment and expansion of healthcare facilities and is associated with fewer hospitals, ambulatory surgical centers, dialysis clinics, and hospice care facilities. It is also associated with fewer hospital beds and decreased access to medical imaging technologies. Residents of CON states are more likely than residents of non-CON states to travel further to obtain medical services and CON laws favor incumbent hospitals in the market for services.
Sources: Ford and Kaserman (1993); Carlson et al. (2010); Stratmann and Russ (2014); Stratmann and Baker (2017); Stratmann and Koopman (2016)
No. CON programs are associated with fewer hospitals overall, but also with fewer rural hospitals, rural hospital substitutes, and rural hospice care. Residents of CON states must drive further to obtain care than residents of non-CON states.
Sources: Cutler, Huckman, and Kolstad (2010); Carlson et al. (2010); Stratmann and Koopman (2016)
Mostly likely not. While early research was mixed, more recent research suggests that deaths from treatable complications following surgery and mortality rates from heart failure, pneumonia, and heart attacks are all significantly higher among hospitals in CON states than hospitals in non-CON states. Also, in states with especially comprehensive CON programs, patients are less likely to rate hospitals highly.
Sources: Stratmann and Wille (2016)
No. There is no difference in the provision of charity care between states with CON programs and states without them, and CON regulation is associated with greater racial disparities in access to care.
Sources: DeLia et al. (2009); Stratmann and Russ (2014)
No. CON regulations have a disproportionate effect on nonhospital providers of medical imaging services and are associated with 14 percent fewer total ambulatory surgical centers.
Sources: Stratmann and Baker (2017); Stratmann and Koopman (2016)
No. By limiting supply, CON regulations increase per-unit healthcare costs. Even though CON regulations might reduce overall healthcare spending by reducing the quantity of services that patients consume, the balance of evidence suggests that CON laws actually increase total healthcare spending.
A full list of Mercatus peer-reviewed research can be found below. You can also visit our update 2020 Research Update, including links to the latest state data
Research on Access
Barriers to Entry in the Healthcare Markets, by Thomas Stratmann and Matthew C. Baker — August 29, 2017
Entry Regulation and Rural Healthcare: Certificate-of-Need Laws, Ambulatory Surgical Centers, and Community Hospitals, by Thomas Stratmann and Christopher Koopman — February 18, 2016
Are Certificate-of-Need Laws Barriers to Entry? How They Affect Access to MRI, CT, and PET Scans, by Thomas Stratmann and Matthew C. Baker — January 12, 2016
Do Certificate-of-Need Laws Increase Indigent Care? by Thomas Stratmann and Jake Russ — July 15, 2014
Research on Quality
Examining Certificate-of-Need Laws in the Context of the Rural health Crisis, by Thomas Stratmann and Matthew C. Baker — July 29, 2020
Certificate-of-Need Laws and Hospital Quality, by Thomas Stratman and David Wille — September 27, 2016
Research on Cost
Do Certificate-of-Need Laws Limit Spending? by Matthew D. Mitchell — September 29, 2016
Can Health Spending Be Reined In through Supply Constraints? An Evaluation of Certificate-of-Need Laws, by James Bailey — August 1, 2016
Research on the Political Economy of CON Laws
The Effect of Interest Group Pressure on Favorable Regulatory Decisions, by Thomas Stratmann and Steven Monaghan — August 29, 2017
On COVID-19
Raising the Bar: ICU Beds and Certificates of Need, by Matthew D. Mitchell, Thomas Stratmann, and James Bailey — April 29, 2020
A Fresh Start: How to Address Regulations Suspended during the Coronavirus Crisis, by Matthew D. Mitchell, Patrick McLaughlin, and Adam Thierer — April 15, 2020
First, Do No Harm: Three Ways That Policymakers Can Make It Easier for Healthcare Professionals to Do Their Jobs, by Matthew D. Mitchell — March 25, 2020
On Community Hospitals and Ambulatory Surgery Centers
Data Visualization: The Impact of Certificate-of-Need Laws on Community Hospitals and Ambulatory Surgery Centers, by Thomas Stratmann and Christopher Koopman — March 15, 2016
On Imaging Services
Data Visualization: Impact of Certificate-of-Need Laws on the Provision of Medical Imaging Services, by Thomas Stratmann and Matthew C. Baker — February 24, 2016
On Access to Care
Data Visualization: How State CON Laws Restrict Access to Healthcare, by Christopher Koopman, Thomas Stratmann, and Mohamad Elbarasse — May 13, 2015
Three Prescriptions for States to Improve Healthcare, by Matthew Mitchell, Anna Mills, and Dana Williams — January 15, 2015
Mercatus scholars regularly provide testimony at the state and federal level. If you'd like to invite a Mercatus scholar to provide testimony, please email our outreach team.
Federal Testimony
- CON Law Letter to Senate HELP Committee, by Matthew D. Mitchell and Anne Philpot. Written testimony submitted to the Senate Health Education, Labor and Pensions Committee — February 28, 2019
- Better Health for More People at Lower Cost, Year after Year, by Matthew D. Mitchell, Anne Philpot, Robert Graboyes, Jared Rhoads, Edward J. Timmons, and Thomas Stratmann. Testimony to Chairman Lamar Alexander — February 28, 2019
State Testimony
Alaska
- Alaska's Certificate-of-Need Program: Lessons from Research, by Matthew D. Mitchell. Testimony before the Alaska Senate Labor and Commerce Standing Committee — April 21, 2021
- Benefits to Patients and Providers in Alaska With the Removal of CON Laws" Darcy N. Bryan, M.D. Testimony before the Alaska Senate Health and Social Services Committee — April 21, 2021
- Alaska’s CON Law: Lessons from Three Decades of Research, by Matthew D. Mitchell. Testimony before the Alaska Senate Health and Social Services Committee — March 27, 2019
- Alaska’s Certificate-of-Need Law, by Matthew D. Mitchell. Testimony before the Alaska Senate Labor and Commerce Committee — February 6, 2018
- The Failure of Alaska’s Certificate-of-Need Laws, by Thomas Stratmann. Testimony before the Alaska Senate Labor and Commerce Committee, Hearing on Repeal of Certificate of Need Program — April 7, 2017
Florida
- Florida’s CON Law: Lessons from Three Decades of Research, by Matthew D. Mitchell. Testimony before the Florida House of Representative Health Market Reform Committee — February 6, 2019
- Do Certificate-of-Need Laws Reduce Spending? by Matthew D. Mitchell. Testimony Before the Florida Health Innovation Subcommittee — January 9, 2017
- Can Health Spending Be Reined In through Supply Constraints? An Evaluation of Certificate-of-Need Laws: Implications for Florida, by James Bailey. Testimony before the Florida Health Innovation Subcommittee — January 9, 2017
Georgia
- The Failure of Georgia’s Certificate-Of-Need Laws, by Thomas Stratmann. Testimony before the Georgia House of Representatives Rural Development Council — September 19, 2018
Illinois
- Illinois’s Certificate-of-Need Laws: Effects on Quality, Spending, and Access to Care, by Thomas Stratmann and Matthew D. Mitchell — June 19, 2017
Maine
- Maine's Certificate-of-Need Program: Lessons from Research, by Matthew D. Mitchell. Testimony before the Maine Joint Committee on Health Coverage, Insurance, and Financial Services — April 6, 2021
Michigan
- Michigan’s Certificate-of-Need Program: Lessons from Research, by Matthew D. Mitchell. Testimony before the Senate Committee on Health Policy and Human Services — January 8, 2020
Mississippi
- Mississippi’s Certificate-of-Need Law, by Matthew D. Mitchell. Testimony before the Mississippi House Public Health and Human Services Committee — September 11, 2017
Montana
- Montana's Certificate-of-Need Program: Lessons from Research, by Matthew D. Mitchell. Testimony before the Montana Senate Committee on Public Health, Welfare, and Safety — March 17, 2021
New Hampshire
- Certificate-of-Need Laws: Implications for New Hampshire, by Christopher Koopman and Thomas Stratmann. Testimony before the New Hampshire House Health, Human Services and Elderly Affairs Committee — January 28, 2015
South Carolina
- South Carolina’s Certificate-of-Need Program: Lessons from Research, by Matthew D. Mitchell. Testimony before the South Carolina Senate Medical Affairs Committee, Certificate-of-Need Subcommittee — May 10, 2021
- Certificate-of-Need Laws: Implications for South Carolina before the South Carolina Department of Health & Environmental Control, by Christopher Koopman, Thomas Stratmann, and Mohamad Elbarasse — June 12, 2015
Tennessee
- Tennessee’s Certificate-of-Need Program: Lessons from Research, by Matthew D. Mitchell. Testimony before the Tennessee Certificate-of-Need Working Group — October 31, 2019
Virginia
- Virginia’s Certificate-of-Public-Need Law: A Comparison with Other States, by Matthew D. Mitchell. Testimony before the Virginia House of Delegates Health, Welfare, and Institutions Committee — April 18, 2018
Washington
- Washington’s Certificate-of-Need Program: Lessons from Research, by Matthew D. Mitchell. Testimony before the Washington State Legislature, House Health Care and Wellness Committee — March 10, 2021
West Virginia
- The Failure of West Virginia’s Certificate-of-Need Program, by Christopher Koopman. Testimony before the West Virginia Senate Health and Human Resources Committee — March 9, 2017