- | Healthcare Healthcare
- | Policy Briefs Policy Briefs
- |
Allowing Compounding Pharmacies to Address Drug Shortages
The COVID-19 pandemic has brought a new era of supply chain challenges. In the areas of energy, semiconductors, cargo ships, and more, once-dependable products and methods of transport are becoming less reliable. These supply chain challenges have caught policymakers off guard, which is understandable because pandemics have unpredictable consequences. However, predictable shortages also are happening in other areas and will continue to happen. In these areas, Americans should be less forgiving if their leaders do not act with deliberateness and foresight. This is especially true in the modern prescription drug market, where shortages are an unfortunate, regular feature.
Drug shortages often result from supply chain interruptions, such as an important drug manufacturer going offline to address a concern about quality. In other cases, drug shortages result from a spike in demand for drugs. For example, the outbreak of COVID-19 led to an increase in demand for drugs administered to patients on ventilators. Although some shortages are outside of the control of regulators, the magnitude and duration of drug shortages can be exacerbated by regulations.
Compounding pharmacies, or compounders, have the wherewithal to step in and address drug shortages when they occur. Compounders come in different forms, but all produce individualized medicines that are tailor-made for patients with specific ailments. Some compounders are like manufacturers in the sense that they produce in bulk, mostly for medical offices and hospitals that need a constant stock of supplies on hand. Other smaller, independent compounders are like local pharmacies. Both have an important role to play in addressing shortages, because compounders can produce drugs when manufacturers of mass-market drugs cannot meet public needs.
The purpose of this policy brief is to explain the role that compounding pharmacies can play in addressing drug shortages and the way their role can be enhanced through smart public policy reforms. The brief begins with some background on the problem of drug shortages in the United States, then provides an overview of the legal framework that governs compounding pharmacies. This framework currently consists of a patchwork of federal and state laws and regulations. Emergency changes made to this system during the COVID-19 pandemic allowed compounding pharmacies to address drug shortages in a manner usually prohibited. However, the ability of compounders to assist in ordinary times is still limited. Moreover, official methods of tracking drug shortages leave much to be desired, which can hinder compounders’ response during both ordinary times and emergencies. The final sections of the brief discuss ways to address these problems, including legislation that has recently been introduced in Congress to make permanent some of the changes made during the pandemic. These sections also discuss potential concerns about compounding pharmacies and their relative safety.
The Problem of Shortages
The definition of a drug shortage is itself subject to some disagreement. The Food and Drug Administration (FDA) defines a drug shortage as “a period of time when the demand or projected demand for a medically necessary drug in the United States exceeds its supply.” An important characteristic of a shortage, according to the FDA, is that “a registered alternative manufacturer will not meet the current and/or projected demands for the potentially medically necessary use(s) at the user level.” Moreover, the words “medically necessary” are particularly important in these sentences, because these are the drugs the FDA emphasizes on its official shortage list. The FDA defines medically necessary drugs as any drug product that is used to treat or prevent a serious disease or medical condition for which there is no other adequately available substitute.
An alternative definition of drug shortage comes from the American Society of Health-System Pharmacists (ASHP), an authoritative private-sector source on drug shortages. This organization defines a drug shortage as “a supply issue that affects how the pharmacy prepares or dispenses a drug product or influences patient care when prescribers must use an alternative agent.” One area of difference between the FDA definition and the ASHP definition is the emphasis the latter places on changes in patient care as a primary determinant of a shortage.
Shortages are a problem for financial and public health reasons. Patient complaints about drug shortages are common, and shortages increase out-of-pocket costs for patients and increase travel time to obtain needed medicines. Shortages also lead to personnel and other costs for hospitals and other medical facilities. Personnel costs owing to shortages have been estimated to be approximately $359 million annually for hospitals, whereas increased expenditures as a result of drug prices rising and paying for more expensive substitutes have been estimated to be about $230 million each year.
Costs are not limited to inconvenience or money. Shortages of insulin or EpiPens, for example, can have serious adverse effects on people with diabetes and allergies, respectively. In the most severe cases, shortages lead to increases in mortality. Increases in hospitalization rates and adverse drug reactions also occur because substitutes can have unintended side effects. One survey of medical professionals (primarily pharmacists) in 2014 finds that 90 percent of respondents had experienced at least one shortage that may have caused a medication safety issue or error in patient care in the prior six months. Another survey of healthcare professionals reports that 35 percent of respondents’ facilities had experienced a “near miss” during the past year owing to a drug shortage.
The exact number of drugs in shortage depends on various factors, including how one defines a shortage. One study based on FDA shortages data counts 917 active shortages of drugs in the year from December 2015 to December 2016. Another study finds that, in 2010, over 240 drugs were either in short supply or were completely unavailable and that more than 400 generic equivalents were backordered for greater than five days. The ASHP reports that 166 new drug shortages occurred in 2019.
As these numbers indicate, the number of shortages varies depending on how one tracks them. Furthermore, it is possible these problems are getting modestly better over time, because by some estimates, counts of drugs that experience shortages seem to be falling. However, the COVID-19 pandemic has revealed that the problem of shortages is far from being eradicated. Thus, a critical question for policymakers is how further progress can be made. Compounding pharmacies can assist during these periods of stress. However, the legal environment in which these businesses operate is complex, so whether they are able to assist when drugs are in short supply ultimately hinges not on their capabilities, but on whether they are allowed to assist under federal law.
Overview of the Legal Framework Facing Compounding Pharmacies
Compounding pharmacies provide custom-made medicines for patients with specific health needs. Compounders necessarily face a different legal and regulatory landscape than do producers of traditional, commercial drugs that are most common in the United States. This makes sense because the cost of going through the FDA approval process for a new drug is far too expensive and time consuming to be practical for individualized medicines that will not be available on a mass-market scale.
Compounding pharmacies come in a variety of forms. Some are like manufacturers in that they produce in bulk, largely for hospital or medical office stock. Others are like local pharmacies, except with the additional capacity to make custom-made drugs. These differences arise partially because separate legal regimes have been established for the two kinds of compounders.
The larger compounders that produce in bulk are named 503Bs (or sometimes “outsourcing facilities”) after the section of the Federal Food, Drug, and Cosmetic Act that establishes their legal treatment. The smaller compounders are known as 503As. A key characteristic of 503As is that these entities, outside of very well-established relationships, have to obtain a patient-specific prescription before filling an order, a requirement that does not apply to the 503Bs. Thus, 503As operate more like traditional pharmacies, dispensing medications for use by known individual patients with a prescription, whereas 503Bs operate more like manufacturers. As a result of this arrangement, the 503Bs must register with and are regulated by the FDA. They have to comply with current good manufacturing practices set by the federal government, and they also face inspections by the FDA. Meanwhile, the 503As come primarily under the regulatory authority of the state boards of pharmacy that regulate pharmacies at the state level.
As a general rule, both types of compounders cannot compound drugs that are “essentially copies” of commercially available FDA-approved drugs, because mass-marketed drugs under the current system must receive premarket approval from the FDA. Thus, compounders are limited to producing individualized medicines. However, given the ongoing occurrence of drug shortages, the FDA and Congress have come to recognize that compounders can play an important role in mitigating these problems and have created a pathway for compounders to produce, in special circumstances, drugs that are similar to FDA-approved drugs.
The specific pathway is outlined in FDA guidance documents. Although 503s cannot compound what are essentially copies of commercially available FDA-approved drugs, when a drug is in shortage, it is not considered commercially available. Then what is considered essentially a copy of an FDA-approved drug in other times can be produced by a compounder during a shortage. This pathway to address shortages works well some of the time, but it leaves much to be desired for several reasons made clear by the COVID-19 pandemic.
First, as will be discussed in more detail later, the FDA’s official drug shortage list—additions to which are what triggers 503s’ ability to compound certain medications—is not comprehensive, partly because FDA drug-shortage staff rely heavily on information reported from manufacturers, and this information can miss shortages that arise for reasons other than production shortfalls.
Second, 503Bs are often not able to revamp production lines rapidly because reorienting product lines takes time. Moreover, these facilities need orders of a sufficient size to justify the expense of making these changes. Thus, smaller shortages may not rise to a level of significance to justify retrofitting assembly lines. A similar issue is that, like any business, 503Bs tend to give priority to their regular customers, so addressing a shortage can take a backseat to filling regular orders.
This is where the 503As could potentially help. Smaller orders needed rapidly can be produced by 503As, which are nimbler than 503Bs—this is not a criticism of 503Bs but simply a recognition of the fact that these entities serve different markets. By their very nature, 503As exist to fill small orders and serve individual patients, whereas 503Bs fill larger orders intended primarily for office stock. The primary impediment to 503As stepping up in these times is the prescription requirement. The FDA consistently affirms this requirement and is hesitant to make it more flexible because the requirement provides a clear legal distinction between 503As and 503Bs. Without the requirement for dispensing of medications only with a prescription, the line between 503As and 503Bs is somewhat blurred. Interestingly, however, the FDA relaxed this requirement during the COVID-19 pandemic.
How COVID-19 Has Changed the Debate
The FDA reports that 86 shortages were ongoing in 2020, compared with 76 in 2019. The FDA exercised regulatory flexibility 110 times in 2020 to address these drug shortages, which related to 78 products. Examples of drugs that went into shortage during this period are drugs related to ventilator use. Acetaminophen and albuterol are two other medicines that saw spikes in demand during the COVID-19 pandemic, leading to shortages.
In response to these problems, the FDA issued guidance in 2020 allowing 503As to produce copies of FDA-approved medications when a medical facility treating COVID-19 patients could not otherwise find drugs from a traditional source or from a 503B. The usual prohibitions against 503As producing versions of FDA-approved drugs, as well as requirements that 503As have a prescription in hand before completing an order, were waived, though pharmacies still had to obtain patients’ identifying information after the fact, within a month, and had to notify their state regulator that they compounded under these conditions.
Interestingly, during this period the FDA was keeping a list of drugs used for hospitalized patients with COVID-19. The list was associated with its guidance allowing compounding of some medications for patients hospitalized with COVID-19. The medicines in the FDA guidance document were not all on the official FDA shortage list, highlighting how the FDA’s official shortage list sometimes requires supplemental lists.
Another hurdle 503Bs face when responding to shortages is that the FDA usually wants 503Bs to start with FDA-approved manufactured products, even though doing so can create unique challenges. For example, US Pharmacopeia finds that some formulations do not work as well when made from a manufactured product, as the FDA wants.
As a result of these complications, the 503B formula development process can be time consuming, leading to delays. Again, 503As can offer a solution. 503As can produce during the time 503Bs are developing formulas or revamping manufacturing lines. 503As produce smaller quantities, and their drugs often have short beyond-use dates, which establish when the product expires such that it must no longer be used. Even if one assumes that 503As are riskier than 503Bs, the potential risks have to be weighed against the risks to patients who are unable to obtain medicines while 503Bs are not producing. Risks posed by any particular 503A will likely be limited owing to its small productions quantities and short beyond-use dates.
As noted earlier, 503Bs can require substantial drug orders before they will service a customer. Thus, these facilities may not respond to smaller shortages. This can especially be an issue in rural areas affected by regional shortages. These more localized shortages may not show up on the FDA drug shortage list either, owing to the FDA’s national focus. A drug shortage list from ASHP, however, is better suited for detecting these kinds of regional issues. However, the ASHP list does not have the same level of policy importance as the FDA list in that adding a drug to the ASHP list does not trigger additional permissions for compounders in the same way as adding drugs to the FDA list.
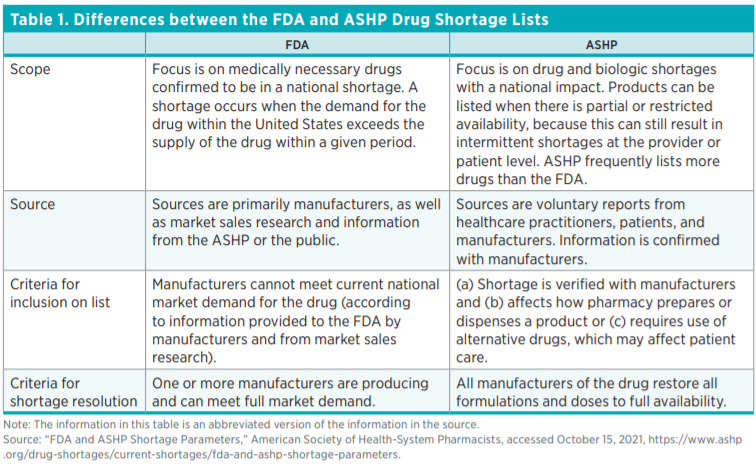
Differences between Drug Shortage Lists
Under the Federal Food, Drug, and Cosmetic Act, manufacturers are required to report manufacturing interruptions to the FDA. The the FDA relies on this information, as well as market research data on drug sales, when making determinations about whether a drug shortage exists. The FDA looks at demand and supply as well as forecasts of these factors, and if estimated demand exceeds supply for the nation, then a drug is considered in shortage.
A supplement to the FDA drug shortage list is that of the ASHP, which has an online portal where its members can report drug shortages. Whereas FDA relies heavily on manufacturers to report issues that arise with production processes, the ASHP gets much of its information from medical professionals, such as pharmacists, in addition to patients and some manufacturers. This more patient-focused perspective may better reflect conditions on the ground.
The number of drugs listed as being in shortage by the ASHP is almost always higher than the number appearing on the FDA list (see table 1). This should not be surprising, given that production changes are only a subset of all the reasons drugs can become hard to obtain. Indeed, this fact became evident during the COVID-19 pandemic, when many shortages arose owing to demand spikes, not supply interruptions.
The ASHP list has several characteristics that distinguish it from the FDA list. First, drugs that are added to the ASHP list are usually first reported by practitioners, so the list is often tracking shortages in real time and is therefore forward looking. The ASHP then verifies practitioners’ reports with drugmakers. A drug is included in the list if its lack of availability affects how a pharmacy prepares or dispenses a product or requires the use of alternative drugs. The ASHP keeps items on the list until they are back to full availability. The FDA list, by contrast, emphasizes drugs deemed medically necessary. It focuses on the national market, using supply and demand data either from the manufacturers or from market sales research, and it assumes that a drug is no longer in shortage when at least one manufacturer is producing that drug and can meet the national demand (see table 1).
Legislative Solutions
Several stylized facts describe the current US drug market with respect to shortages. First, periodic drug shortages are a recurring feature of the market. Second, the process that has been laid out by Congress and the FDA to allow 503s to compound in response to shortages has not fully resolved the problem. Third, the COVID-19 pandemic has forced a policy response to this situation. That response may offer insights as to how the current legal landscape can be reformed to make further improvements.
Likely in response to this set of facts, legislators in Congress have been looking to draw lessons from changes made during the COVID-19 pandemic. A bipartisan bill introduced in the House of Representatives in 2021, H.R. 3662, would codify some of the FDA’s emergency permissions that it granted to 503As during the pandemic. Specifically, it would make permanent changes related to responding to urgent-use and shortage drugs when those drugs are unavailable from other sources.
If passed, the legislation would do several things. First, it would expand the exemption from drugs deemed “essentially copies of a commercially available drug product” to include drugs on the ASHP drug shortage list. This may be an improvement, because the ASHP list combined with the FDA list is probably a better barometer of drug shortages than the FDA list in isolation. Second, the legislation would carve out a predictable pathway for 503As to address drug shortages , one with a less stringent prescription requirement. That pathway would involve a hospital or other purchaser of drugs first seeking an FDA-approved drug from an ordinary source. If the drug could not be procured via that route, the licensed prescriber could then go to a 503B for a drug with the same active ingredient. If that route were to fail, it could approach a 503A.
This exact set of steps would have to be followed and appropriate records maintained. Moreover, 503As would have to procure records that identify the patient to whom the drug products were administered within a week of the medication being received or the patient being discharged. This record would be attached to the corresponding drug order.
In short, H.R. 3662 would codify the practices that the FDA itself has endorsed as a practical response to the COVID-19 emergency. This approach makes sense because it creates a predictable framework that stakeholders can anticipate, rather than having to rely on impromptu guidance from the FDA. Allowing 503As to resolve drug shortages when all other potential options run out should help both in times of emergencies, like the COVID-19 pandemic, as well as when shortages arise in noncrisis situations.
Potential Concerns
Critics of compounding pharmacies express concern about patient safety. One concern is that, because 503As are not directly regulated by the FDA and because both they and 503Bs produce drugs that differ from mass-market FDA-approved drugs, these producers are more dangerous than other drug manufacturers.
The most notable piece of evidence in support of this claim is an outbreak of fungal meningitis that took place in 2012 and 2013 owing to contaminated drugs produced by the New England Compounding Center, located in Framingham, Massachusetts. The Pew Research Center has catalogued US illnesses and deaths associated with compounded or repackaged medications from 2001 through 2019. Pew has identified 1,562 adverse events, including 116 deaths during this period, that were associated with compounding errors or potential errors.
More than one-half of the adverse events and about two-thirds of the deaths catalogued by the Pew Research Center stem from the single New England Compounding Center case. Without minimizing the seriousness of these adverse events and deaths, one can acknowledge that this event is fortunately an outlier in terms of the health harms it caused and in terms of the extent of fraud and criminal activity on the part of the firm in question. In addition to criminal sentences that were imposed in response to that event, Congress passed the DQSA in 2013. The DQSA is what created the 503A-503B distinction, detailing a process by which larger outsourcing facilities (503Bs) would be regulated by the FDA and have to conform to current good manufacturing practices, whereas smaller compounders (503As) would be regulated primarily at the state level.
Former FDA Commissioner Scott Gottlieb suggested in Congressional testimony that, in response to the law, the FDA had hoped more 503As would convert to 503Bs, thereby bringing more compounders under FDA oversight. However, the considerable compliance costs associated with making that transition act as a barrier to the FDA’s goal (though the FDA has also expressed a priority of preserving the traditional 503A designation). The FDA estimates that it would cost a large or a medium-sized pharmacy about $600,000 to become a 503B facility and that it would cost a large manufacturer about $1 million. It seems likely that these high compliance costs are hindering the FDA’s efforts to increase the number of 503Bs.
Thus, a kind of limbo now exists in the regulatory system. Compounders want to be regulated in a manner that ensures the safety and reliability of their drugs. Moreover, everyone seems to accept 503As as a legitimate part of the compounding landscape that can be relied on to serve Americans’ medication needs. It serves no one to force all small compounders into the current FDA-regulated framework, given that the high compliance costs would drive many of these small entities out of business. The New England Compounding Center incident should not be forgotten, and patient safety must be a top priority, but the DQSA also leaves many unanswered questions. Congress’s job must be simultaneously to clarify the unresolved issues in the DQSA, preserve the role of small compounders and create flexibility for them to respond to shortages, and create a safe environment for patients. It is a tough balancing act, but a solution is now becoming evident.
Conclusion
The reforms suggested in this brief are meant to serve as last-resort options. There are risks associated with compounding pharmacies, but risks must be balanced with benefits. The FDA has tried for years to address the problem of drug shortages, and although some progress has been made, the COVID-19 pandemic has revealed that the country is still far from achieving the optimal solution.
When the alternative is no patient access to drugs, there is an easy choice: let compounders provide patients with the medicines they need. Currently, regulatory barriers stand in between patients and drugs in times of distress, but Congress and the FDA can solve these problems. Fortunately, good options are available, as the FDA’s own emergency actions during the pandemic make clear. A window is opening for reform, and Congress now has both the tools and the information it needs to act. The question now is whether it will do so.

