- | Healthcare Healthcare
- | Policy Briefs Policy Briefs
- |
Public Health in Rural States: The Case against Certificate-of-Need Laws
Certificate-of-Need Laws Artificially Restrict Providers of Care in Rural Areas
Despite the advances of medicine of the past few decades, individuals in rural communities continue to face barriers to access to healthcare. While hospital consolidation and provider shortages present real challenges, an underrated barrier to access to care stems from legacy laws that were implemented almost 50 years ago: certificate-of-need (CON) laws. These laws exist in 37 states (including 12 of the country’s 20 rural states) and put up artificial barriers to the provision of care by allowing regulators to decide whether new services are needed in a given geographic area. In practice, healthcare industry incumbents are heavily influential in the process and tend to block potential competitors from entering local markets. A new study by the Mercatus Center at George Mason University controls for social risk factors including race, education, and poverty status and finds that CON laws are associated with higher readmission rates and more emergency department (ED) visits among Medicare beneficiaries in rural areas. CON laws in rural states are also associated with hundreds of dollars of additional expenditures and higher ambulance spending per Medicare beneficiary.
CON Laws Do Not Achieve Their Goal
Since CON laws were first implemented, research has shown that they have never achieved their intended purpose of reducing or controlling healthcare spending. State governments, with the help of local industry leaders, were to determine whether a new service was necessary to meet the needs of the population, with the objective being to limit the number of available healthcare services to prevent overutilization. The federal government encouraged such efforts in the early 1970s by giving states subsidies for setting up CON laws. It did not take long for policymakers to realize that CON laws were not achieving their goal, and in 1986, the federal government removed the corresponding financial incentives. Several states repealed their CON laws, but many did not. Today, 37 states have a CON program that applies to anywhere from 1 to 29 healthcare devices, facilities, and services. Studies confirm what economic theory makes clear: all else being equal, restrictions on supply lead to increases in cost. Not only have CON laws backfired, but now ample evidence shows that CON laws have resulted in unintended side effects such as lower healthcare quality and restricted access to needed services, especially in rural states and counties.
Rural States with CON Laws Fare Worse
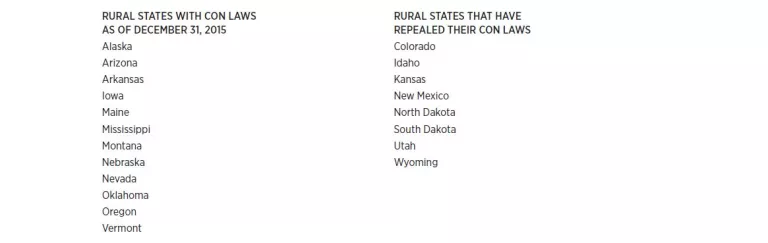
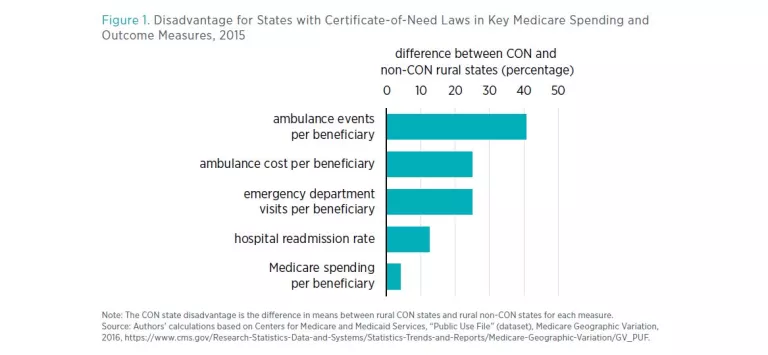
These states have varying socioeconomic characteristics that are associated with poor health outcomes. Still, when the researchers control for age, race, poverty status, and education, rural states with CON laws fare worse both in terms of health outcomes and healthcare spending than their non-CON counterparts (see figure 1).
Before controlling for the earlier-mentioned socioeconomic variables, CON states are associated with higher spending per Medicare beneficiary and higher readmission rates, more ED visits per 1,000 beneficiaries, and higher ambulance spending. The disparities remain when including those controls: CON rural states spend $295 more per Medicare beneficiary and have 1.2 percentage point higher readmission rates, 35.1 more ED visits per 1,000 beneficiaries, and $2.54 higher ambulance spending per beneficiary than do non-CON rural states. These are common metrics of potentially preventable—and often wasteful—spending, often linked to limited access to care that could have better managed chronic conditions and prevented the need for acute care.
Far from helping states save money and provide much-needed services to Medicare beneficiaries, CON laws have the opposite effect in rural areas and lead to worse outcomes than in states that do not have CON restrictions. States that wish to direct dollars toward high-value care and enhance clinical outcomes should consider pursuing some of the following reforms.
States Can Solve the Problem, and the Federal Government Can Help
The most straightforward and effective way of simultaneously improving health outcomes and reducing healthcare spending is for rural states to repeal CON laws. Attempts to do so have often been met with fierce political opposition, however, as incumbent hospitals and service providers act as powerful special interests. Therefore, we propose other pathways to gradually repeal CON laws.
Partial Repeal of the Most Harmful CON Laws
CON states often have CON requirements for various types of procedures and services. Legislators should consider the full list of CON requirements in their state and determine which ones impose the heaviest burden on the state’s residents.[5] For example, some CON laws are more likely to affect vulnerable patients, such as CON laws for drug and alcohol abuse treatment centers (found in 24 states), CON laws for psychiatric care facilities (found in 28 states), and CON laws for intermediate-care facilities for those with intellectual disabilities (found in 28 states). Certain CON requirements apply to services that are unlikely to be overprescribed, which means that those who seek to provide such services are not looking to build unnecessary capacity that will drive up costs. Examples include CON laws for neonatal intensive care units (found in 22 states), CON laws for burn care units (found in 14 states), and CON laws for hospice care facilities (found in 18 states). On similar grounds, other types of CON laws to consider removing are those that apply to inexpensive procedures and small investments, such as home healthcare services.
Phased Repeal through Sunset Clauses, Contingent Action, or Increases in Approval Rates
When immediate repeal is infeasible, CON law repeal can be spread over time via different policy strategies: sunset clauses, or automatic phase-out timelines, can be included in bills so that CON laws eventually expire. Three rural states, Idaho, Kansas, and Wyoming, added sunset clauses to their CON laws when the federal government removed its incentives for states in the late 1970s, and their CON programs subsequently expired. In 2012, New Hampshire approved a sunset effective 2015. Similarly, a CON state could make its CON laws contingent on policy decisions in neighboring states, so that its CON laws would go away should a neighboring state eliminate its CON laws also. Another route would be for states to mandate that CON boards approve a steadily growing share of CON applications, culminating with the approval of all applications, effectively amounting to a CON law repeal.
Administrative Relief for CON Applicants
If the earlier-mentioned forms of repeal are infeasible, states with CON laws can make the process of obtaining a CON less onerous by reducing fees and simplifying reporting criteria. They can also improve applicants’ odds of success by removing certain criteria, including nonduplication, utilization thresholds, and geographic requirements.
Increased Transparency in the Approval Process
Applicants face a number of uncertainties when seeking a CON, including uncertainties regarding the amount of time the process will take and the total costs thereof. The outcome of the process may also be influenced by incumbents’ efforts to challenge the application and by potential financial ties of CON board members to incumbent businesses. Transparency on all these fronts would minimize uncertainty and help applicants maximize their odds of approval.
Centers for Medicare and Medicaid Services Can Support Rural States’ Efforts
Through the Center for Medicare and Medicaid Innovation, the Centers for Medicare and Medicaid Services has shown support for innovation in the delivery of high-quality healthcare services to Medicaid and Medicare beneficiaries. The presence of CON laws limits the number of services available to individuals in rural communities. Additionally, it also prevents providers from developing innovative services for patients by putting up high, artificial barriers to the provision of care. If spending differences are caused by CON laws, then CMS could reduce payments in states that have CON laws to give them incentives to scale down requirements.
Conclusion
Although the negative effects of CON laws have been well-known for decades, new evidence about their elevated effect on rural states adds urgency to the need to remove restraints on providers in areas with poor health outcomes and high healthcare spending. At stake for residents of rural areas is not only their contribution to healthcare spending but also their health and livelihood.
This policy brief summarizes a variety of options for policymakers wishing to remove regulatory barriers to the care on which rural residents depend—primarily suggesting a full repeal of CON laws but, in recognition of legislative and political hurdles, offering feasible alternative fixes.

