- | Medical Innovation Toolkit Medical Innovation Toolkit
- | Regulation Regulation
- | Data Visualizations Data Visualizations
- |
Does FDA Funding Increase Drug and Medical Device Innovation?
The US FDA receives funding through the general fund and user fees. Additional funding comes from the regulated industries. Specifically, the drug industry funds FDA through the Prescription Drug User Fee Act (PDUFA), and the medical device industry funds FDA through the Medical Device User Fee Act (MDUFDA). Both acts are considered a success for requiring FDA to improve approval time for drugs and devices. However, decreased approval times have not resulted in more drug and device innovation.
INTRODUCTION
The US FDA receives funding through the general fund and user fees. Additional funding comes from the regulated industries. Specifically, the drug industry funds FDA through the Prescription Drug User Fee Act (PDUFA), and the medical device industry funds FDA through the Medical Device User Fee Act (MDUFDA). Both acts are considered a success for requiring FDA to improve approval time for drugs and devices. However, decreased approval times have not resulted in more drug and device innovation.
In fact, the same number of products are still submitted for approval to FDA. They are just approved more quickly. FDA does not have an incentive to actually increase innovation—its only incentive is to meet its MDUFA and PDUFA approval times to keep its funding flowing. The expense of putting drugs and devices through this system is almost unimaginable. The cost of bringing low- to medium-risk 510(k) medical devices to market averages $31 million, $24 million (75 percent) of which is dedicated solely to attaining FDA approval within an average of about six months. Any significant improvement to the device requires reapplication. For higher-risk medical devices where there may be significant health gains, the costs are about $94 million, $75 million (80 percent) of which is dedicated to attaining FDA approval.
For drugs, the situation is much worse. It costs an average of $2.6 billion simply to get a drug through the FDA process and onto the market. This does not include postmarket monitoring, the terms of which are laid out by FDA upon approval. These costs have increased from about $1 billion between 1983 and 1994.
In addition, the primary laws governing devices and drugs are now 40 and 50 years old, respectively. These laws, in conjunction with other incentives, attenuate progress in the device and drug arenas. As one congresswoman describes it, “Health research moves at a rapid pace, but the federal drug and device approval process is in many ways a relic of another era.” Yet we continue to increase the funding and authority for FDA and assume that we will somehow boost innovation in medical products (drugs and devices) despite the growing obstacles. This has not happened.
FDA has grown in both resources and statutory authority, and to continue those increases, it must meet user fee goals and avoid bad publicity.
FDA FUNDING
Concerns Relating to User Fees
FDA and industry initially opposed user fees, first considered in the 1950s. Early discussions focused on drugs, for which FDA began getting user fees in 1992. Earlier objections cited the disproportionate burden user fees would impose on “the poor and the elderly” through higher drug prices. FDA’s Center for Drug Evaluation and Research (CDER) maintained that user fees for Investigational New Drugs would function as a tax and discourage innovation.
There was also considerable concern about FDA’s sluggishness in approving drugs relative to counterparts in other countries—the “drug lag.” A key reason industry began to support user fees was that “the [New Drug Approval] review times were so long, and the cost of an NDA was there- fore so large, that if an NDA was approved even one month quicker, it would reduce the cost of the NDA by more than the user fee.” These fees have been widely declared a success, particularly by FDA, in reducing “the total time it takes to make decisions.” However, speedier approvals do not necessarily equal speeding up innovation. In fact, establishing performance goals that avoid unintended consequences, or that satisfy more fundamental goals like increasing the rate of innovation, is notoriously difficult.
Economist Robert Heilbroner provided an apocryphal story about managing incentives through central planning in the Soviet Union. He wrote that “If the output of nails was determined by their number, factories produced huge numbers of pinlike nails; if by weight, they produced smaller numbers of very heavy nails.” The ultimate goal of producing more nails that are actually useful is never achieved.
Heilbroner’s point is not that incentives created by government do not work. They do, but they do not necessarily incentivize the desired outcome. Although it appears that PDUFA and MDUFA have met their approval goals with respect to timeliness, just as with the satirical nail factory, the ultimate goal of more medical product innovation is not achieved.
FDA’s Budget Increases
FDA funding increases have been largely uninterrupted for the last 15 years. Fees from the drug and devices industries help FDA’s funding grow more rapidly than that of agencies that depend on general funding alone. FDA’s 2017 requested budget increase for drugs and devices (no increase requested for biologics) is $26,294,000. The bulk of that increase (87 percent) would come from user fees. Figures 1, 2, and 3 show the growth in FDA budgets.
Figure 1: Total Funding (FDA Overall)
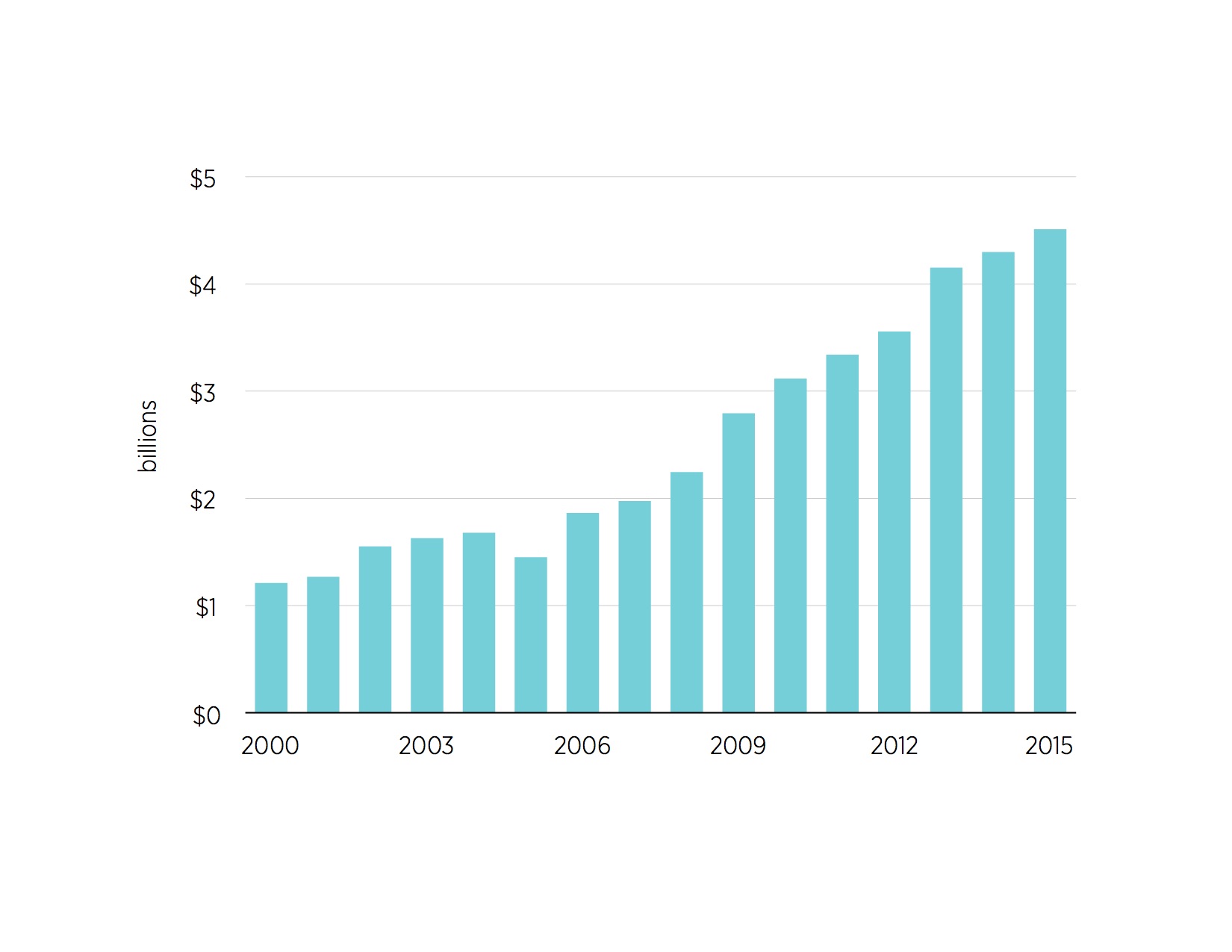
Figure 2: Human Drug Funding (2000-2015)
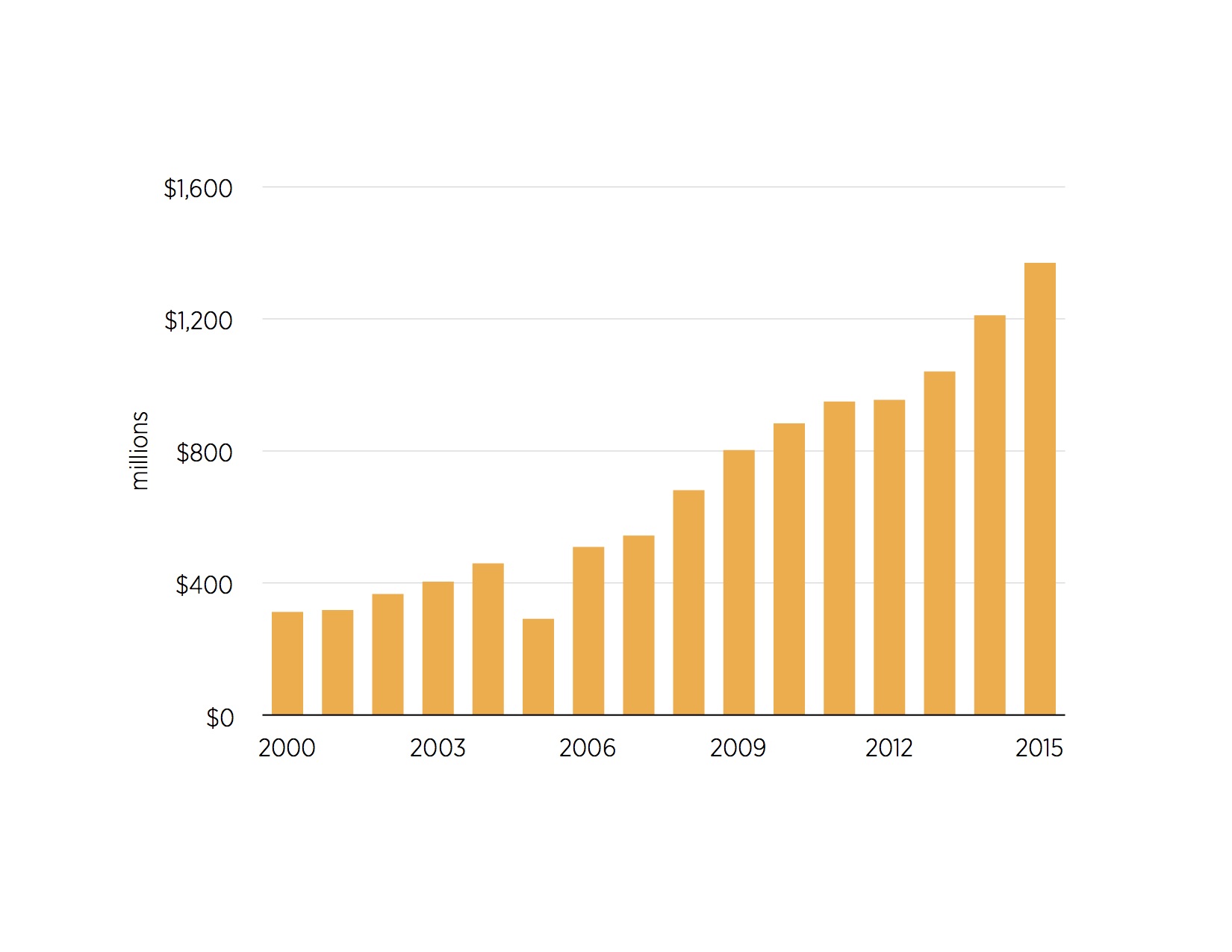
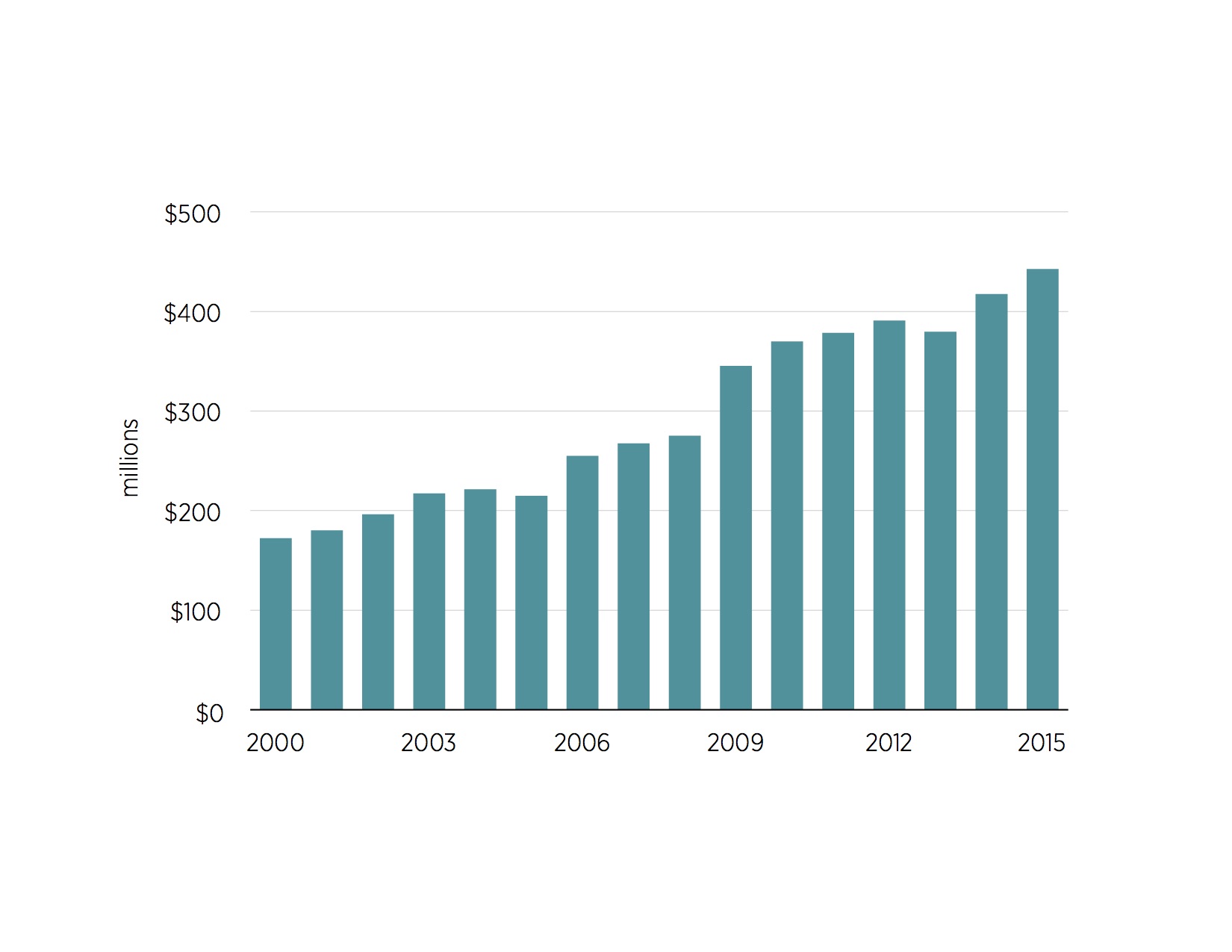
Figure 3: Devices and Radiological Health Funding (2000-2015)
Related Content
- | Medical Innovation Toolkit Medical Innovation Toolkit
- | Regulation Regulation
- | Working Papers Working Papers
Health Options Foreclosed: How the FDA Denies Americans the Benefits of Medical Research
- | Medical Innovation Toolkit Medical Innovation Toolkit
- | Regulation Regulation
- | Data Visualizations Data Visualizations
More FDA Spending Does Not Necessarily Mean Better Results
- | Regulation Regulation
- | Research Papers Research Papers
US Medical Devices: Choices and Consequences
- | Medical Innovation Toolkit Medical Innovation Toolkit
- | Regulation Regulation
- | Data Visualizations Data Visualizations
Maze of FDA Regulations Slows Medical Innovation to a Crawl


