- | Regulation Regulation
- | Public Interest Comments Public Interest Comments
- |
HHS’s Innovative New Sunset Regulation
Background on the Rule
The Department of Health and Human Services (HHS) is proposing a regulation that would build sunset provisions into its existing and future rulemakings and force more rigorous retrospective review of its regulations and their impacts on small businesses. The proposed regulation is a welcome development, and this comment is intended to provide evidence for why more retrospective review is critical at the current juncture as well as how the current proposed rulemaking can be improved before being finalized.
HHS is proposing what would effectively be a retrospective review requirement for its regulations, giving emphasis to their impact on small business. When such a review is not conducted, regulations expire according to a predetermined schedule. Similar sunset reviews are undertaken at the state level as well in other nations, and the threat of expiration seems to stimulate more careful review than otherwise would occur. The potential benefits from this proposed rulemaking, particularly for small businesses and the general public, are large and are likely to exceed the proposed rule’s modest costs.
How the HHS Rule Will Likely Work in Practice
The department is proposing to add a provision to various sections of the US Code of Federal Regulations (CFR) that contain HHS regulations. These provisions would force periodic review of regulations for their impacts on small businesses, in accordance with section 610 of the Regulatory Flexibility Act (RFA) of 1980, which requires periodic review. HHS’s proposed review process would work in two steps: (1) HHS would assess whether a particular regulation (defined as a section of the CFR) has a significant impact on a substantial number of small entities; if yes, then (2) HHS would conduct a more in-depth review of the regulation.
If the assessment and review (when required) are not undertaken, then the relevant regulation expires 2 years after the sunset regulation being proposed becomes effective, 10 years after the regulation being reviewed became effective, or 10 years after the regulation being reviewed was last assessed and reviewed under the proposed sunset regulation, whichever is latest.
In practice, this would mean that going forward, regulations issued by HHS would expire 10 years after enactment unless they were assessed and reviewed in accordance with the RFA. RFA assessment and review would delay the scheduled expiration for another 10 years, at which point the rule would need to be assessed again, and so on. Existing regulations on the books older than eight years will sunset two years following implementation of this regulation (because for these older regulations, this is the latest of the three deadlines) unless assessed and reviewed, if necessary. HHS estimates that roughly 12,400 of the 18,000 regulations it has on the books are older than 10 years, the “vast majority” of which would need to be assessed within 2 years as a result of this regulation. HHS also estimates that approximately 10 percent of its regulations have a significant economic impact on a substantial number of small entities (meaning more in-depth reviews will be required for these regulations) and predicts that this number could increase as rules are assessed.
Bipartisan History of Retrospective Review
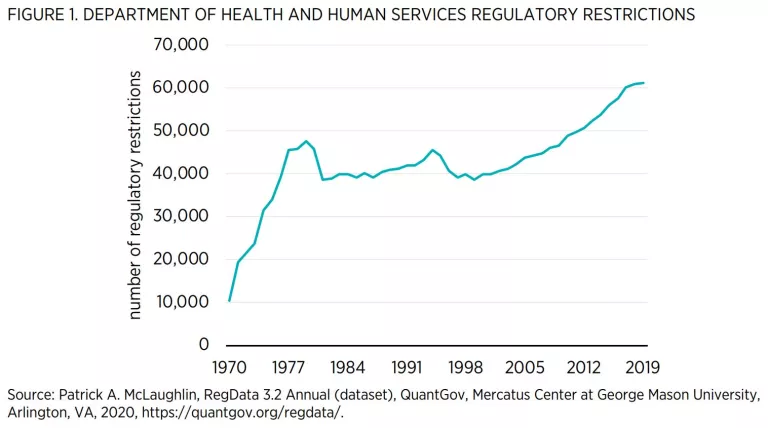
As HHS goes to great lengths to note in the preamble to the notice of proposed rulemaking, there is a long bipartisan history of support for retrospective review of federal regulations. HHS cites various executive orders from Presidents Carter, Clinton, and Obama that encourage looking back on regulations. Republican presidents have also prioritized reviews (with the current president being the most recent example). Yet to date, most observers note that these kinds of reviews have failed to become institutionalized at federal agencies. RegData, a dataset produced by the Mercatus Center at George Mason University, measures the volume of regulations by counting regulatory restrictions: instances of the terms “shall,” “must,” “may not,” “prohibited,” and “required,” which can signify legal constraints and obligations. RegData shows that despite efforts to review regulations over the years and to reduce regulatory burdens, the total number of regulatory restrictions that have been issued by HHS continues to grow year after year (see figure 1), except for two brief periods around 1980 and during the mid-1990s (perhaps as part of deregulatory efforts).
Why might meaningful retrospective review have failed to take hold at federal agencies, despite numerous efforts from presidents of the two major political parties? One reason is incentives. There is no penalty for an agency when it ignores RFA periodic review requirements. Keith Belton and John D. Graham note that “one of the best-kept secrets in Washington, D.C. is that Congress has already required a retrospective review process for each federal regulation under the [RFA], at least for those regulations that impact small businesses. This provision of the RFA has not been implemented with any rigor, in part because the task would be enormous and in part because there is no penalty if an agency ignores the RFA.” (The provision of the RFA alluded to by Belton and Graham is section 610.)
Contra Belton and Graham’s claim, however, retrospective review need not be an enormous task. The work can be divided up over time. Even if it were an enormous task, that fact would not be an excuse not to review regulations. If reviewing regulations is too enormous a task for the regulating agency, imagine how difficult it must be for regulated entities to make sense of all the restrictions they have to comply with. Yet Belton and Graham are correct that periodic review has not taken hold at federal agencies.
HHS, citing a Congressional Research Service report, notes that “[w]ithout some type of enforcement of the review requirement, agencies are unlikely to conduct many more reviews than have occurred pursuant to Section 610.” Michael Greenstone, who was chief economist on President Obama’s Council of Economic Advisers, has recommended sunset provisions as an enforcement mechanism to spur retrospective review, which is the approach taken in this rulemaking. Greenstone’s recommendation demonstrates that there is bipartisan support not just for retrospective review, but for sunset provisions as a mechanism to spur such review.
A Breakeven Analysis of the Proposed Rulemaking
HHS estimates the total cost of this regulation to be between $10,066,719 and $25,781,696 over 10 years. These costs include mostly personnel costs associated with tasking employees with reviewing regulations. The costs of this regulation are somewhat front-loaded, meaning that the first two years of review will appear exceptionally expensive as a result of having to make up for many years of disappointing compliance with the RFA. But once conducted, not all those costs are likely to recur. HHS estimates that the cost in the first two years will be between $7,638,722 and $19,101,091.
The benefits of the regulation are difficult to anticipate fully, because they could stem from modifying nearly any regulation under HHS’s purview and therefore could come in almost any form. However, there are a number of reasons to believe that the benefits of this rulemaking will vastly outweigh the costs just described.
First, as HHS notes in its press release for the regulation, HHS’s own budget exceeds $1 trillion annually. Healthcare spending more generally constituted about 17.7 percent of GDP in 2018, or $3.6 trillion. If, as a result of its review, HHS were to find cost savings worth 0.0025 percent of departmental spending or 0.0007 percent of national spending, the regulation would pay for itself and pass a cost-benefit test at the higher end of cost estimates. These are miniscule fractions, and given that healthcare spending is projected to take up nearly 20 percent of the economy in the future (in large part owing to growth of Medicare spending), the potential to find cost savings in the system is likely to keep increasing. Small changes to HHS regulations can result in enormous cost savings, given the volume of healthcare spending from HHS and in the United States generally.
Another way to look at this issue is to consider the cost of HHS’s stock of existing regulations as a means to identify the cost savings potential of periodic review. Several studies have shown that regulations are costly and, moreover, that these costs are often regressive. One recent study that uses RegData estimates the annual cost of federal regulation to be $4 trillion in 2012 when there were 1,033,847 regulatory restrictions on the books. This estimate suggests a cost per restriction of $3.87 million. In 2012, HHS had 50,801 restrictions in the CFR. If the average cost of an HHS restriction is comparable to the estimated average cost of a restriction in the 2012 CFR generally, then HHS regulations cost about $200 billion in 2012, and the removal of three to seven regulatory restrictions could cover the cost of the entire proposed regulation over 10 years. Whereas it should be emphasized that this is a back-of-the-envelope calculation, its basic conclusion is likely to hold true: the removal of a handful of regulatory restrictions with significant economic impacts could easily pay for this regulation (perhaps many times over).
Tellingly, the Office of Management and Budget (OMB) has also deemed this regulation to be economically significant. The definition of an economically significant regulation is one “having an annual effect on the economy of $100 million or more in any one year.” Given that the highest annual cost for the regulation is unlikely to exceed $10 million, OMB seems to expect benefits to exceed $90 million in at least one year, which dwarfs even the high end of 10-year cost estimates for this regulation by a margin of more than 3 to 1.
Importantly, beyond cutting regulatory burdens, the scheduled assessments and, when necessary, reviews of existing HHS regulations afford HHS the opportunity to keep regulations up to date with modern trends. Yes, HHS would have the opportunity to terminate obsolete regulations that are no longer fit for purpose or that are judged to be ineffective. But in addition, the provisions in this proposed rule would give HHS and the public a reliable framework and a set of tools to continually keep regulations up to date with evolving circumstances.
One study notes that, although sunsets are not a panacea, they can “add flexibility and dynamism to the principle of legal certainty and assist it in keeping up with the rapid changes of society and technology. By terminating laws when they cease to be effective or experimenting on a small scale with novel legislative approaches, instead of frequently correcting permanent laws; legislators can incorporate new information, legislate better and avoid frequent legal revisions.”
Finally, it is also worth reiterating that HHS is already required to conduct periodic reviews under section 610 of the RFA. If HHS were fully complying with the spirit of the law, there would likely be no costs of this rulemaking (nor benefits). It is only because HHS’s current compliance with the law is so disappointing that this regulation is necessary.
Potential Concerns about This Regulation
HHS should not be surprised if some interest groups express concern about this regulation. Many regulations bestow privileges upon narrow constituencies by creating barriers to entry in their industry. Such regulations tend to be anticompetitive and also slow growth. Expect industry incumbents to fight to preserve their existing anticompetitive privileges. However, such anticompetitive regulations are also exactly the kinds of rules that are likely to disproportionately burden small businesses, because small businesses are often the new entrants such regulations are intended to keep out. The fact that industry incumbents prefer not to review anticompetitive regulations is not evidence that there is no need for a review.
Some regulations emerge from lengthy negotiations between industry and advocacy groups. HHS has asked for comment on “regulations of particular importance that HHS needs to ensure are Assessed or Reviewed so they do not expire.” Industry groups concerned about such rules should bring them to HHS’s attention in response to this request for comment. However, HHS should keep in mind that just because revising these rules could be costly and time consuming does not mean these rules should not be reviewed in order to better understand their effects.
In addition, just because a regulation is agreed upon by both industry and advocacy groups does not necessarily mean that the regulation is in the public interest. There is a well-documented phenomenon known as “Bootleggers and Baptists,” whereby advocacy groups, nominally claiming to act in the public interest, collude with industry to enact regulations that benefit both groups. Whereas sometimes such regulations benefit the public at large, too often these regulations direct benefits to these concentrated interest groups while dispersing costs across the entire population.
Again, HHS should expect to face resistance to reform from those who benefit from the status quo and to find those who stand to benefit from reform the most—the public—to be less organized and less inclined to participate in the regulatory process. HHS should keep in mind always that it is the public that stands to gain the most from its sunset proposal, even if members of the public are not actively lobbying the agency to act in their interests.
A final argument that HHS may hear against reform relates to uncertainty. Business and advocacy groups may argue that the proposed sunset regulation creates hard-to-quantify uncertainty, which adds to the costs of this rulemaking. However, the sunset provision here primarily serves to ensure that HHS reviews regulations as required by the RFA, which means that if HHS were currently complying with the RFA in a satisfactory manner, there would be little additional uncertainty stemming from this rulemaking. Moreover, this regulation is unlikely to unleash significant uncertainty, as evidenced by the numerous instances of sunset provisions working effectively in the states as well as in other countries. Several jurisdictions sunset regulations in a more systematic way than has been proposed by HHS.
Indiana, New Jersey, and North Carolina have sunset policies for regulations, which seem to work quite well. California, Colorado, and Texas are examples of states that have a sunset process for entire boards, commissions, and agencies. Colorado’s process is one of the oldest in the country and has been in place since the 1970s. If sunsetting individual regulations creates significant uncertainty, it would be hard to imagine why states as large and diverse as Texas and California would create a sunset process for entire agencies.
Furthermore, sunset provisions form a key part of the regulatory process in places such as Australia, Canada, and the United Kingdom. In Australia, since the passage of the Legislation Act of 2003, all regulations (known as legislative instruments), with some exceptions, automatically expire 10 years after enactment unless parliament acts to extend the period or a replacement instrument is adopted. The Australian Federal Register of Legislation (the equivalent to the Federal Register in the United States) maintains the sunset dates for qualifying legislation. In the United Kingdom, regulatory bodies can include sunset clauses in regulations. If they so choose, regulations would sunset usually within seven years, and departments are encouraged to track and review regulations before the expiration date.
Some states even have an annual sunset for their entire administrative code. Although the clause is rarely allowed to be exercised, there nonetheless is always the possibility it will be exercised. In fact, two states (Idaho and Rhode Island) allowed their entire regulatory codes to sunset in recent years. Both sunsets took place smoothly and without any notable negative repercussions. In Idaho’s case, the regulatory code expired on very short notice, whereas in the case of HHS’s rules the public will be aware years in advance of regulations potentially expiring. It seems likely that if a state is able to sunset its entire administrative code on a few months’ notice with minimal disruption, then potentially sunsetting regulations with 10 year’s notice (or 2 year’s notice for relatively older regulations) would not create significant uncertainty.
In the same vein, many major federal laws have sunset clauses. Notable among these are the Patriot Act, enacted in the aftermath of the 9/11 terrorist attack, and tax laws that were passed as part of the budget reconciliation process under the Byrd Rule in the US Senate. It stands to reason that the uncertainty that would surround HHS regulations would be negligible compared with major laws such as the Tax Cuts and Jobs Act of 2017 and the Jobs and Growth Tax Relief and Reconciliation Act of 2003, which have a wider reach than most HHS regulations and do not seem to have caused major disruption to the economy.
Moreover, HHS can maintain a public list of regulations that are due for assessment and review to reduce any accompanying uncertainty. As recommended by the Organisation for Economic Co-operation and Development, HHS can dispel some of the concerns about uncertainty by maintaining and publishing a schedule of regulations that are due for assessment and review. This type of “programmed review” would give both HHS and the public ample time to prepare for the review.
Finally, it is worth noting that even regulations without sunset clauses are uncertain to the extent that Congress can repeal the authorizing laws at any time. Thus, all public policy is uncertain to some extent. This hardly constitutes a reason for forgoing periodic reviews.
Recommendations for Improvement
HHS has asked for feedback on several provisions of the rulemaking. This section is intended to provide responses to HHS considering these requests.
- HHS is asking for feedback on whether it should review a different set of regulations than those that have a significant economic impact upon a substantial number of small entities.
The emphasis on small businesses in this rulemaking seems entirely appropriate for several reasons. First, there is general recognition that regulations disproportionately burden small businesses. For example, a 2010 study by the Small Business Administration finds that in 2008, small businesses faced annual regulatory costs of $10,585 per employee, which was 36 percent higher than the regulatory costs facing large firms ($7,755 per employee). Second, there is bipartisan support for supporting small businesses, as evidenced by the passage of the RFA and the Small Business Regulatory Enforcement and Fairness Act. Third, the RFA requires periodic review of regulations, the aim of the present regulation. That said, while conducting its reviews, HHS should identify those regulations that would be deemed significant or economically significant under executive order 12866. This practice could be useful for reporting purposes as well as for more in-depth analysis later. At present, keeping the core focus of reviews on small businesses is likely to be most practical for the reasons outlined here.
- HHS is asking for feedback on whether reviews should consider, in addition to factors listed in 5 U.S.C. § 610, whether regulations remain cost effective or cost justified. If so, how should HHS determine if a regulation is cost effective, cost justified, or both?
HHS should consider performing a cost savings analysis for regulations receiving a “review” under the proposed regulation (or perhaps for that subset of reviewed regulations that are deemed significant or economically significant). Such analysis would include estimates of the costs, cost savings, and the net cost savings of the regulation. This approach has the advantage of being simple and therefore relatively easy to produce rapidly. It may also avoid some of the challenges discussed in the next section regarding retrospective analysis.
- HHS is asking for feedback on what baseline and what time frame to use when conducting an analysis of an existing regulation.
HHS has several options when conducting analyses under this proposed rulemaking. One route is simply to conduct an ex ante analysis of how the regulation is likely to perform going forward compared with the baseline scenario of what would happen if the regulation were allowed to expire under the sunset provision. This approach has several advantages. First, HHS already produces ex ante analyses, so this would not be a dramatic departure from present practices. Second, the analysis could still include a backward-looking component to the extent that data collected on the performance of the regulation in the past could be used to forecast how the regulation would perform in the future. In this sense, the ex ante analysis will still have a retrospective element. Finally, it is how a regulation will perform in the future that should ultimately determine whether the rule should continue or be amended in some way. (With regard to the time frame of the analysis, this decision is likely to vary by regulation just as it does in other regulatory impact analyses.)
That said, for ex ante analysis, many assumptions are uncertain at best. Ex post, HHS would likely have access to more accurate data about the actual performance of the regulation and would therefore be able to improve the original cost-benefit estimates for the regulation. Retrospective analysis of regulations is a feature of regulatory systems in a number of countries including Australia, Canada, and the United Kingdom. For example, in Canada, there is a cabinet directive that, among other things, discusses a life-cycle approach to regulations. One of the steps in this life cycle is the regular review of enacted regulations.
Therefore, a second, slightly more complicated option would be to conduct a backward-looking cost-benefit analysis for some existing regulations. To do this, first HHS should select a reference year from which to evaluate the regulation. This would logically be the year when the regulation was implemented or the year when the new analysis is taking place. The analysis would likely look at how the regulation performed relative to the baseline of what would have happened either in absence of the regulation or relative to the rule as it stood before it was last amended in a significant way. The comparison may need to take place relative to multiple baselines given the uncertainty of the counterfactual scenario. (OMB also recommends considering multiple baselines in some instances.)
In a retrospective cost-benefit analysis, some issues, such as discounting, become even more counterintuitive than usual. It is our belief that discounting consumption does not have a sound economic basis retroactively (for example, it makes sense for nonpecuniary health and mortality benefits in the past to receive the same weight as present benefits). However, it still makes sense to convert investment dollars into their shadow prices to account for the opportunity cost of capital (because losing one dollar of investment in the past is more costly than losing one dollar of investment in the present, owing to reinvestment). These issues are complicated and there may be no consensus among economists about how to deal with them. Again, a cost-savings analysis may be more practical and efficient and less controversial.
- HHS is asking for input on how best to integrate plans for retrospective review into new rulemakings.
HHS can identify data up front that it will use to track the progress of the regulation and commit to continually collecting the same kinds of data over time. This action will make evaluation of rules and programs easier later on and improve accountability because the public will have a clearer sense of what a regulation is supposed to achieve and can monitor HHS’s progress.
Conclusion
HHS’s new sunset regulation is a major achievement and can serve as a model for other agencies in the future. The regulation represents a major effort to institutionalize retrospective review and analysis at one of the biggest, most important US federal agencies. If successful, this would not just be a significant accomplishment, it would be historic.
Additional details
Securing Updated and Necessary Statutory Evaluations Timely
Agency: Department of Health and Human Services
Comment Period Opens: November 4, 2020
Comment Period Closes: December 4, 2020
Comment Submitted: December 4, 2020
Docket No. HHS–OS–2020–0012
RIN: 0991–AC24

