- | Healthcare Healthcare
- | Policy Briefs Policy Briefs
- |
For Greater Healthcare Access, License Physicians Like Pilots
The United States spends more on healthcare than any other nation—in absolute terms, as a percentage of gross domestic product, and per capita. Nevertheless, it has problems of access and quality, which pose problems for patients, providers, payers, and policymakers. Those in rural areas, inner cities, and Native American communities face special challenges of access, as do linguistic minorities and residents of particular states and regions.
In this brief, we address (a) problems of access; (b) the way state licensure and scope-of-practice laws contribute to these problems; (c) the way politics underlies these public policies and the resulting access problems; (d) the mechanics of healthcare licensure; (e) the mechanics of pilot licensure; (f) the similarities and differences between healthcare professionals and pilots; and (g) some policy options by which states can apply the lessons of pilot licensure to the healthcare professions.
We choose pilot licensure as a model for healthcare licensure for two reasons. First, the pilot licensure model offers lessons that can be readily applied to healthcare. Second, piloting and healthcare have many strong similarities. Both require a mastery of complex technical systems with thousands of moving parts; both operate in turbulent environments where sudden, unexpected events can pose grave dangers to customers; and both use diverse skillsets. For example, the skills required for neurosurgery are vastly different from the skills required for dermatology or radiology, just as the skills required to operate a Boeing 747 at night are vastly different from the skills required to fly a single-engine Cessna by day.
The Problems of Access
Large segments of the US population live in federally designated medical and dental shortage areas. There are many possible causes for these asymmetries in access to healthcare. As we discuss later, healthcare licensing regulations by the states are an important component of this problem. Just when the COVID-19 pandemic began, USA Today reported that 218 US counties do not have a single physician. Some regions are critically short on particular specialists, which can be lethal for patients. In many areas, regions must wait days, weeks, even months for appointments. And when appointments are secured, they may be all too brief because the limited supplies of providers are rushed to care for other patients. Forecasts suggest that, left unchecked, problems of access will increase considerably in the coming years as America’s population increases, as swelling numbers of elderly people demand greater amounts of healthcare (a particularly significant trend), and as educational institutions fail to produce enough providers to meet rising demand. As we argue in this brief, a significant part of the problem relates to licensure, with solutions to be found in changing the rules of licensure.
How State Laws Constrict Access
A big part of the problem is that politicized state licensure and scope-of-practice laws and regulations unnecessarily restrict the supply of care by constraining who can provide healthcare and which services can be provided. Both the Obama and the Trump administrations recognized the problems caused by these laws and regulations, including unnecessary restrictions on the services that certain classes of providers (e.g., nurse practitioners [NPs], physician assistants [PAs]) can provide. Medical licensure is ostensibly designed to protect the American public from practitioners who are incompetent, unethical, or dishonest. But in practice, this politicized regulatory system restricts qualified individuals who are capable of providing healthcare and for whom there is ample demand. Scope-of-practice laws limit the services that some healthcare providers could otherwise provide given that their training and qualifications fully meet the technical requirements established for the provision of those services.
What Aviation Can Teach Healthcare about Access: Get Politics Out of Licensing
The legal and regulatory processes for licensing or certifying healthcare providers and airplane pilots are radically different. The number of pilots and the services a particular pilot may provide are less constrained by regulation and political processes. Medical licensure and scope-of-practice laws, by contrast, are highly politicized, with artificial constraints imposed by state legislators and regulators. Federal immigration restrictions and state laws unduly limit the ability of international medical graduates to obtain licenses in the United States. They also prohibit NPs from performing procedures that are part of their training. These limitations play a significant role in creating gaps in healthcare workforce supply, making it difficult to meet the changing demands of patients.
By contrast, there are no limits on the number of people who may obtain licenses to fly airplanes. Pilots can receive training in foreign and domestic flight schools, foreign and domestic military settings, or individual tutoring. They must meet relatively objective criteria regarding skill and competence. And, unlike physicians, pilots must periodically subject themselves to reevaluation in order to maintain their licenses.
The Supply of Healthcare Is Arbitrarily Limited by State Politics
While gaps in access to healthcare proliferate and deepen, state laws needlessly and arbitrarily limit the number of healthcare providers and needlessly restrict what they do and how they do it. The following sections describe some of the remediable problems generated by this political process.
Limits on Medical School Slots and Residencies
There are only two sources of medical doctors (MDs) in the United States: accredited American medical schools and international medical schools, whose graduates are referred to as IMGs (international medical graduates). The supplies of American medical school graduates and IMGs are both unduly constrained by states.
The number of American-trained physicians is constrained by the number of accredited medical schools and by those schools’ class sizes. These limits on the number of diplomas awarded each year places a hard ceiling on the number of American-trained physicians who can eventually be licensed. A single private organization—the Liaison Committee on Medical Education (LCME)—is the only agency each state legislature recognizes that can accredit medical schools. The LCME is affiliated with the American Medical Association and controlled by MDs. Because states grant only MDs exclusive license for an unrestricted practice, other professions can train their students to learn only what their scope of practice permits. Moreover, NPs, PAs, optometrists, and other healthcare professionals are ineligible for advanced specialty training for which their work experience might otherwise prepare them, because the relevant postgraduate programs require an MD degree as a prerequisite for acceptance. The recent exception is osteopaths, who had been forbidden hospital privileges for years. It took many lawsuits and their laudable service in Vietnam to break down the professional barriers. If the reforms we envision in this brief were adopted, existing professions and potentially innovative new professional boards could ameliorate the constraints.
Barriers to International Medical Graduates
America imports large numbers of IMGs, who train in medical schools outside of the United States. Some IMGs are Americans whose applications were rejected by American medical schools, but most are foreign-born physicians and currently make up 25 percent of America’s physician workforce. They are especially important in alleviating the shortage of primary care providers in rural areas.
However, states place undue obstacles in the way of well-trained, competent IMGs who wish to practice in America. State licensing regulations generally require all IMGs to take additional training in various accredited postgraduate programs regardless of their experience, length of training, or competence. IMGs also have more difficulty finding postgraduate training programs that accept them. Once again, states grant a private entity, closely associated with organized medicine and run by MDs, to determine the size and number of accredited training programs for IMGs. (This entity is the Educational Commission for Foreign Medical Graduates.) For many IMGs this is an unnecessary waste of time, but there is currently no way to discriminate between those who need further training and those who do not.
Conflation of Credentials and Competency
In general, American medical training is based on a fixed-time, variable-learning model. Students proceed through medical training at a rigidly synchronized pace built around a semester schedule. Effectively, they are judged by the amount of time spent in training, rather than by their mastery of the topics at hand. Of course, they must achieve passing grades in their coursework, but this fixed-time learning model means that students emerge from their coursework with widely varying levels of competency in particular areas of study. This model directly contrasts with the fixed-learning, variable-time models typically employed in airplane pilot training and pioneered by Toyota. Under the “Toyota Kaizen Methods,” an individual must completely master each training segment before moving along to the next. Hence, each person proceeds at a different pace through training segments.
Those who complete their medical education are granted unrestricted licenses to practice. They may perform any standard medical services, including surgery, regardless of their levels of competency in the particular procedure. And, though most states require MDs to undergo periodic continuing medical education, MDs are not reevaluated for competency. Loss of license occurs only under egregious circumstances. Again, this situation directly contrasts with the one for airplane pilots, who must undergo periodic reexamination.
Protectionist Policies with Respect to Out-of-State Licensees
In 2002, a surgeon in New York was able to remove the gall bladder of a patient in France using a surgical robot over a high-speed terrestrial network. Yet in many or most states, laws prevent physicians in other states from merely consulting with patients over the internet, unless they are licensed in the patient’s home state. This limitation has been suspended during the COVID-19 emergency, but in some states these constraints may be reinstated, along with their excessive costs to patients.
Undue Limits on Competent Nonphysicians
States make it difficult for nonphysicians to alleviate the shortage of healthcare providers. NPs, PAs, nurse anesthetists, midwives, pharmacists, physical therapists, psychologists, and optometrists all have significant skills that could be useful in meeting the needs of currently underserved patients. But since exercising those skills is considered practicing medicine, scope-of-practice limitations prohibit nonphysicians from offering services for which they are fully competent unless specifically permitted in their states. Only physicians are permitted to practice medicine, unless specifically exempted by statute.
States differ in what is permissible. NPs may write prescriptions and practice independently in Arizona. In California, NPs have to practice under the supervision of a physician via collaborative practice agreements. In Florida, they may not prescribe medication unless a physician nominally supervises them.
Scope-of-practice limitations and mandatory collaborative practice agreements also make it difficult to establish innovative delivery systems. For example, retail clinics such as CVS’s MinuteClinics have been a big success in providing walk-in primary care services to patients with acute needs. They are less expensive and far more convenient than emergency rooms, and they can be a godsend in areas that lack primary care physicians. Studies have shown that, when these clinics are staffed by PAs or NPs, they reduce costs while maintaining medical outcomes similar to those of facilities staffed by physicians. Yet in some states, laws concerning scope-of-practice and collaborative practice agreements effectively prevent their operation.
Politicized versus Nonpoliticized Licensure
The restrictions on medical education, IMGs, teaching models, out-of-state licensees, and non-MDs emerge from a highly politicized process. If NPs wish to expand their scope of practice—to perform, say, vasectomies—the determination on that expansion lies with the state legislature. Scientific evidence indicates that NPs perform procedures for which they have been trained as safely and successfully as physicians. Such evidence, however, becomes irrelevant in bitter political turf battles between NPs and MDs. When a legislature denies such an expanded scope of practice for NPs, it arbitrarily constrains the supply of healthcare, which reduces access to healthcare. A recent report enumerates the relative scope-of-practice restrictions in each state, but the data were collected before the pandemic, and the regulatory situation in the states has been in flux throughout the pandemic.
Whenever licensing is decided by political bodies in this manner, the diploma becomes a surrogate of competence. MDs may legally do anything without asking permission, even if they have never done it before. Diplomas are limited to the number specified by the profession. Potential entrants to the profession from nonfavored groups are considered incompetent until politicians decide otherwise. They may not be permitted to practice at the top of their license.
In turn, whenever licensing is decided by a committee of experts, competence gets appraised according to demonstrated knowledge and skill. No limitations need to be placed on the number of people entering the profession. Once professionals are certified, no authority can prevent them from practicing at the top of their license. They are considered competent unless they break the rules or demonstrate professional negligence or incompetence. We recognize that the line between politicized and depoliticized is a matter of degree, but the distinction is meaningful nevertheless.
In the next section, we compare the politicized process of healthcare licensure with the nonpoliticized process of licensing airplane pilots.
Pilot Certification as Model for Nonpoliticized Healthcare Licensure
We distinguish between politicized and nonpoliticized licensure. With politicized licensure, the structure of the healthcare workforce—i.e., who can practice medicine, whether non-MDs can practice at the top of their licenses, and whether non-MDs must be supervised by MDs—is determined by a political body with no special expertise in healthcare, rather than by a body of experts and practitioners making decisions based on training, skills, and competence.
By contrast, the process by which airline pilots are certified is nonpoliticized—in fact, it is similar to getting a driver’s license. Aspiring airline pilots enter flight schools. Classroom work is needed to learn the rules of the “road.” Student pilots must learn aeronautical theory, navigation, and flying in controlled airspace. They have to take written examinations to prove that they have mastered these subjects. Prospective airline pilots must acquire fundamental skills such as flying by instrument and controlling multi-engine aircraft. Before they can take their final flight exams with Federal Aviation Administration (FAA)–certified instructors, they will have accrued over a thousand hours of actual flight experience in a broad range of weather conditions. They will have proven in simulators that they can handle emergencies. Once certified, no authority can prevent them from exercising all their skills; they can practice at the top of their license.
There are no legal limits on the number of flight schools or the number of pilots in training. Legislatures do not directly regulate the supply of pilots, and consequently, the market for pilots is more competitive and responsive than the market for healthcare providers.
How Physicians Are Similar to Airplane Pilots
Airplane pilots and physicians (along with other healthcare providers) bear strong similarities. Both professions require knowledge of extraordinarily complex systems; one would be hard-pressed to say whether the human body (and the environment around it) is more or less complicated that a Boeing 747 (and the environment around it). Both pilots and physicians must master highly technical processes. They must be prepared for life-threatening contingencies at any moment. The year 2009 saw two radically different aviation outcomes: Captain Chesley Sullenberger saved 155 lives by successfully landing US Airways Flight 1549 in the Hudson River, whereas five months later, 228 lives were lost when the crew of Air France Flight 447 lost control when the speed sensor froze, unable to guide the plane through unusually turbulent conditions.
The technologies of medicine and aviation change over the years, and safety depends upon maintaining currency in the field. Success or failure depends not only on the pilots or physicians, but also on the colleagues and machines around them and their ability to evaluate the integrity of the ecosystem that they inhabit.
How Physicians Are Different from Airplane Pilots
Of course, physicians and pilots are different in many ways as well. The relationship between physician and patient is generally more intimate than that between pilot and passenger, though there are exceptions. (A radiologist likely has less familiarity with those whose scans she reads than the pilot of a corporate jet has with the CEO whom she ferries.)
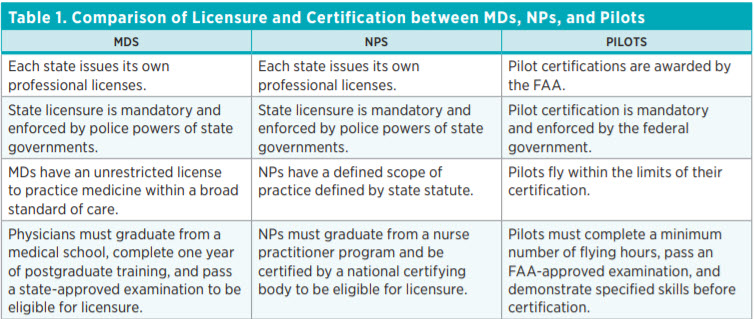
Table 1 lists differences and similarities among MDs, NPs, and pilots, some of which we have described earlier. Physicians are often protected from competition from competent out-of-state providers and in-state nonphysician providers (e.g., PAs and NPs). Barring egregious circumstances, a medical license is conferred for life, whereas pilots must undergo periodic reexamination. Physicians can perform medical services for which they have no particular training, whereas pilots are limited to those activities in which they are certified. And importantly, the pedagogical methods are radically different: fixed-time, variable-learning for doctors versus variable-time, fixed-learning for pilots. Most of these differences are institutional and not intrinsic to the professions.

Learning from Aviation: Policy Options for Healthcare Licensure
In the previous sections, we have focused on two general points: (a) licensure and scope-of-practice laws and regulations unnecessarily constrict the supply of healthcare in a time when access to care is a growing challenge, and (b) the institutions that train and license airplane pilots offer a model for restructuring the training and licensing of healthcare professionals. The following are some public policy options that could move healthcare education and licensing in the direction of pilot education and licensing—from a more politicized process to a less politicized one in which markets and competing professional boards determine the size of the healthcare workforce and precisely which services particular professions or individuals can offer.
The current form of American medical education was set in 1910 with the American Medical Association’s Flexner Report. The report recommended standardizing admissions standards and curricular design across medical schools. One can debate whether the model was appropriate for 1910, but arguably, in 2021, it unnecessarily prolongs the process of medical education, poses a barrier to innovative pedagogical models, raises the cost of education, and bars competent individuals from expanding the healthcare workforce. Potential remedies for these unintended consequences include the following:
- Extend reciprocity and full practice privileges to licensees from other states. In 2019, Arizona passed legislation allowing physicians and other healthcare professionals licensed in other states to begin practicing immediately upon relocating to Arizona and going through a registration process. Arizona’s broad-reaching law is a unilateral lowering of interstate barriers that does not require reciprocity from other states. While the Arizona model is preferrable because it does not require additional expense on the part of the practitioner or bureaucracy on the part of the state, another option would be to join the Interstate Medical Licensure Compact. According to the compact, a physician licensed in one member state has the ability to treat patients in any of the other member states.
- Recognize diversity of educational venues and teaching models. As noted earlier, pilots train in a variety of institutions, including private US flight schools, private overseas schools, US armed forces, foreign armed forces, and one-on-one training from tutors. Similarly, in some states, licenses to practice law can be acquired via education at accredited law schools, unaccredited law schools, or apprenticeships (referred to as “reading law”). Similar diversity could characterize pathways to healthcare licenses. At present, the accreditation process for medical schools essentially homogenizes the pedagogic model and curriculum. Clayton Christensen, Jerome Grossman, and Jason Hwang, among others, have noted that the prevailing teaching model in medical training is fixed-time, variable-learning. Diversity of educational venues and models could encourage teaching institutions to experiment with the Toyota Kaizen methods in training.
- Allow more diversity of applicants. Entry-level training institutions could have more discretion in deciding which qualifications are required for acceptance to their programs. They may choose to accept applicants who pass tests of knowledge and skill administered by third parties other than colleges. These could include high schools, community colleges, the military, or private healthcare facilities. Training institutions could allow students to fill in gaps in knowledge (e.g., organic chemistry) after admission. Before the Flexner Report standardized medical education in the United States, African-American medical schools allowed entering medical students to take catch-up courses that had not been offered at historically black colleges and universities. After the Flexner Report, such students became ineligible for admission to medical schools, and five of the seven existing African-American medical schools closed. Programs could allow students to meet prerequisites using prior certifications from a variety of accrediting organizations. Postgraduate training programs, formerly open only to MDs, may also opt to change their prerequisites for prior training to qualify providers who have been certified by non-MD boards. This has already been done for osteopaths.
- Eliminate special obstacles to licensure of IMGs. In a regime of competency tests for all aspiring licensees, IMGs could be subjected to precisely the same competency tests as American-trained physicians. In a system where the roles of education and certification are separated, where competency exams replace specific pedagogical models and degrees, and where certification entities compete, there need not be any special barriers to IMGs. Laws like Arizona’s unilateral recognition of all other states’ licenses would lower the barriers to IMGs as well as to domestically trained physicians. Joining the Interstate Medical Licensure Compact would also lower the barriers to IMGs, though not as significantly as an Arizona-type law. It is worth noting that if one state adopts such competency-based standards and joins the Interstate Medical Licensure Compact, that would seemingly lower the barriers to IMGs across the states belonging to the compact.
- Allow multiple certification boards to determine scope of practice for non-MD providers. In some states, this idea already has a toehold, in that osteopathic physicians have a separate licensing board from allopathic physicians (MDs). Boards for NPs, PAs, and other non-MDs could determine the scope of practice for their diplomates. This could include widening the scope of practice for those providers who acquire certifiable skills beyond what is required for their license. For legal precedent, one can look to maritime law and EU law on approval of medical devices. From the 1750s to today, multiple entities (maritime classification societies) have been empowered to certify the safety of ships. And in the European Union, multiple state-recognized entities (notified bodies) are entitled to approve medical devices. For states, part of the challenge would be to establish criteria for approving of new (and existing) certification entities.
To be clear, we do not call for federal preemption. The policies we suggest can be implemented by individual states and, if circumstances dictate, rescinded later. We do not recommend imposing the pilot model of training, certification, recertification, or sanction upon MDs. The legacy profession should be left to maintain the status quo or evolve as it sees fit. Disruptions will occur simply by initiating the suggested reforms, and if proven beneficial, they will be embraced by the general population. MDs can choose to follow whichever path seems most profitable to them. Disruptions that occur with the greatest impact arise from the ground up by unforeseen innovators and cannot be predicted in advance. One has only to remember how Uber’s ridesharing innovation revolutionized the taxi industry’s regulatory landscape to appreciate the power of a competitive market.
Conclusion
The current politicized system of licensure and scope of practice was adopted in the early 20th century, largely in response to lobbying by the American Medical Association. The system that arose is comparable to the medieval guilds that limited the number of individuals who could practice certain professions. As with those guilds, admission to the profession (licensure) is a lifetime grant, barring egregious behavior. By coincidence, aviation first appeared around the same time as the current system of medical licensure, but pilot education and certification went in a very different direction—a far more competitive environment.
The United States is in an opportune moment for reform. Without substantial changes, the shortfall of healthcare professionals will grow considerably worse in a fairly short period of time. The American Association of Medical Colleges projects a shortfall of 139,000 physicians by 2033. At the same time, the COVID-19 pandemic forced the state and federal governments to adopt exigencies for the duration of the crisis. States rapidly overturned the licensing restrictions by, for example, allowing physicians licensed in one state to treat patients in other states—in person or via telehealth. Scope-of-practice restrictions were lifted, allowing PAs, advanced practice registered nurses, and other professionals to offer broader ranges of services and, in many cases, to do so without the previously required physician supervision.
The question is whether the states will rise to the challenge, make some of these emergency policies permanent, and adopt even broader reforms that make competency the central consideration in answering the question, “Who may provide a service?” Aviation offers a licensing model that healthcare may well wish to emulate.

