- | Healthcare Healthcare
- | Policy Briefs Policy Briefs
- |
How Certificate-of-Need Reform Can Increase Access to Higher-Quality, Lower-Cost Healthcare in Vermont
More than 60 percent of Vermonters live in rural areas, and for over 30 years, access to quality healthcare in these areas has been hindered by the state’s certificate-of-need (CON) laws. These laws require those who wish to open new healthcare facilities, expand existing facilities, or even purchase new equipment to first obtain permission from a regulator. The regulator—in this case, the Green Mountain Care Board—is charged with assessing whether or not the proposed service is needed by the community. In other states and other industries, this need would be determined by the provider’s assessment of the potential profitability of the venture.
The process of obtaining permission can take years and can cost would-be providers tens of thousands or even hundreds of thousands of dollars. Decades of research on the effects of CON laws suggest that these regulations limit access to care, raise the costs of care, and diminish the quality of care.
CON Laws: Background and Current Situation
In 1974, Congress passed the National Health Planning and Resources Development Act, which made certain federal funding conditional upon the implementation of CON laws. All but one state, Louisiana, passed CON laws as a result. The stated intent of the law was to improve access to care, lower costs, encourage the use of hospital substitutes, and increase quality. CON laws work by requiring healthcare providers that wish to offer a new service in the state to first obtain an authorization (i.e., a certificate of need) by demonstrating a need for the service. In light of research suggesting that CON laws were ineffective, Congress repealed the federal mandate in 1986. Today, however, 35 states, including Vermont, still have such laws, and there is overwhelming evidence that they harm patients and contribute to high healthcare costs.
CON Laws Harm Patients and Providers and Drive Up Costs
The advocates of CON laws claim that by asking providers to demonstrate the need for new services, only those services that benefit the community—that meet patients’ medical needs and are cost effective—will be offered. The half-century-long experience with CON laws suggests that this is not how they work. Because several states have repealed their CON laws and because they have done so at different times, researchers have been able to compare outcomes in CON and non-CON states. Using sophisticated econometric techniques that control for other possible confounding factors, their research suggests that CON laws are associated with limited supply, higher prices, and lower-quality care.
On the supply side, throttling the rate at which new services are introduced and making that process costlier seems to have resulted in fewer options for patients to choose from. For example, researchers have found that CON laws are associated with fewer dialysis clinics, fewer hospice care facilities, fewer hospital beds, and fewer hospitals and ambulatory surgery centers in both urban and rural areas. Residents in CON states must travel farther to obtain care, are more likely to leave their states in search of care, and are less likely to utilize medical imaging services. Finally, researchers have found that there are greater racial disparities in the provision of care in CON states than in non-CON states.
Consistent with economic theory, as CON laws have restricted supply, they have also been associated with higher costs of care. Research also finds that the quality of care suffers under CON laws, resulting in more postsurgery complications and higher mortality rates.
Unfortunately, CON laws have achieved none of the stated objectives that policymakers intended, which vindicates Congress’s decision to do away with the federal mandate 32 years ago. Instead, research suggests that the rules exist to protect incumbent providers from competition rather than to protect patients or taxpayers. Antitrust authorities at the federal Department of Justice and the Federal Trade Commission have long taken the position that these rules are anticompetitive. And recent research has found that political campaign donations are statistically significantly associated with CON approval.
Despite the evidence that has accumulated against them, these outdated regulations continue to unnecessarily limit access to care, and Vermont is worst in class.
Vermont's CON Regime is More Restrictive than Any Other State's, But Substantial Improvements Can Be Made
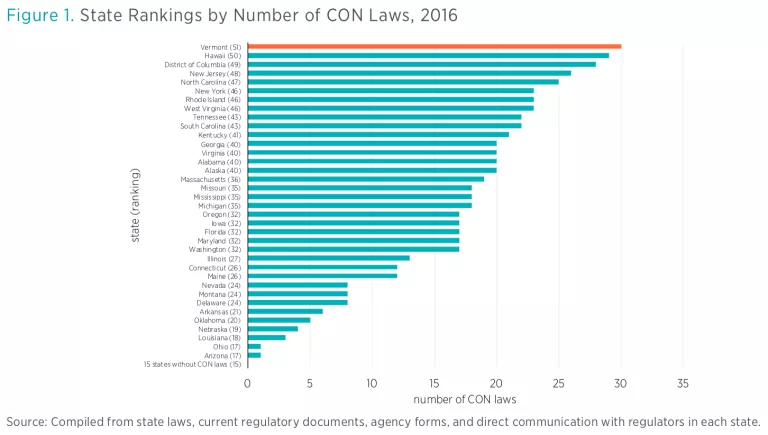
Vermont currently requires a certificate of need for 30 different services (see figure 1). That is more than any other state. Extrapolating the results from studies comparing CON and non-CON states, scholars at the Mercatus Center at George Mason University estimate that a Vermont without CON laws would likely experience the following differences in cost, access, and quality of care:
• Costs:
Healthcare spending per person per year: approximately $228 less
- Healthcare spending per physician per year: approximately $68 less
• Access:
Approximately 6 more hospitals, including 5 in rural areas, where there are currently 13
Approximately 36.4 percent more MRIs performed by nonhospital providers
Approximately 70 percent more CT scans performed by nonhospital providers
• Quality:
Approximately 4.5 percent greater patient satisfaction
Lower mortality rates from pneumonia—approximately 11.6 percent rather than
12.1 percent
Approximately 5 percent fewer deaths from postsurgery complications.
Conclusion
CON laws are outdated regulations that reduce the availability of providers, raise the costs of healthcare, and jeopardize the health of patients in Vermont. Research suggests that scaling them back would lead to a healthier population, while simultaneously lowering healthcare expenditures, with best results obtained by repealing them entirely. Please find more information about the benefits of scaling back CON laws in Vermont on the Mercatus Center’s website.