- | Healthcare Healthcare
- | Policy Briefs Policy Briefs
- |
The Medicare Physician Fee Schedule: Overview, Influence on Healthcare Spending, and Policy Options to Fix the Current Payment System
The Medicare Physician Fee Schedule (MPFS) determines how much healthcare providers are reimbursed for the services they provide to Medicare beneficiaries, and it has considerable influence on healthcare spending in the United States. These rates, set at the federal level by the Specialty Society Relative Value Scale Update Committee (RUC), do not accurately capture the value of the services provided and create misaligned incentives by rewarding providers for delivering care on the basis of the volume and intensity of services and, conversely, by discouraging the provision of valuable but undercompensated services.
In this paper we give an overview of how Medicare sets reimbursement rates for physician services, and we discuss the major flaws in the current administrative pricing system. We also offer several policy recommendations, including the use of more accurate data to set prices for Medicare Part B services in the short term, as well as fully utilizing the potential of Medicare Advantage to accelerate the transition away from fee-for-service (FFS) and administrative pricing to alternative payment models (APMs) and value-based healthcare.
The United States spends more on healthcare—in total and per capita—than any other developed country. Healthcare spending has consistently grown faster than GDP year after year. According to recent projections of National Health Expenditures, the annual growth in national health spending is expected to average 5.1 percent over the decade from 2021 to 2030 and to reach nearly $6.8 trillion (19.6 percent of GDP) by 2030.
Economists have offered various explanations for this alarming growth in healthcare costs. The United States ranks in the bottom half of the Organisation for Economic Co-operation and Development countries on health-service utilization; the late Uwe Reinhardt and his colleagues compellingly argued that the prices paid for services3 are behind the increase in healthcare spending. Medicare Part B’s administrative pricing formula influences the price of physician services across the healthcare system and has played an important role in raising the cost of healthcare in the United States.
How can Medicare price setting be reformed to reduce growth in healthcare spending? We explain how Medicare Part B pricing works and propose adjustments that would make those prices better reflect the costs of the services. We ultimately recommend moving away from administrative pricing by expanding Medicare Advantage and establishing competitive bidding within Medicare Advantage to accelerate the transition to value-based care.
MEDICARE’S BASIC STRUCTURE
As of October 2021, 64 million Americans were enrolled in Medicare, the federal government’s public insurance for the elderly and certain younger people with disability status. Medicare is made up of four parts. Part A employs a capitation system that pays a fixed amount per day for inpatient hospital stays, skilled-nursing-facility stays, and hospice care, as well as a predetermined payment rate for a 30-day period of home healthcare for Medicare enrollees. Part B generally covers provider services as well as other goods and services, such as durable medical equipment, ambulance transportation, X-rays, lab tests, and certain prescription drugs that require administration by a physician. Parts A and B are often referred to as original or traditional Medicare. In Part C, also known as Medicare Advantage, private insurers contract with the federal government and are paid a fixed amount per person to provide all the Medicare benefits that are covered in traditional Medicare. Most plans include additional benefits, such as dental, vision, and hearing coverage; fitness; and, often, drug coverage. Part D, also known as the Medicare prescription-drug benefit, covers most outpatient prescription drugs and is offered through private companies either as a stand-alone plan (for those enrolled in traditional Medicare) or as part of a set of benefits included with a Medicare Advantage plan. Although rising drug prices have received considerable attention of late, in 2020 retail prescription drugs represented just 8 percent of total healthcare expenditures, while physician services accounted for 20 percent.
In this brief, we explore how Medicare Part B sets prices and how those rates influence private insurance. We also consider obstacles to negotiating prices and implications for policy making.
HOW THE CENTERS FOR MEDICARE AND MEDICAID SERVICES SET REIMBURSEMENT RATES FOR PHYSICIAN SERVICES
As of September 2020, less than one percent of nonpediatric physicians have opted out of Medicare. Of the providers who have not opted out, 97 percent are participating providers and accept the Medicare-allowed prices as full payment. The remainder are nonparticipating providers: they get 95 percent of the allowed amount from Medicare and are allowed to bill patients for an additional amount not to exceed 15 percent of the allowed amount. Physicians who opt out of Medicare can establish private contracts with Medicare beneficiaries and charge them whatever they wish.
FFS, Resource-Based Relative Value Scale, Current Procedural Terminology, and the MPFS
Medicare Part B uses an FFS payment system that reimburses providers a set amount for each service with payment rates (the allowed amount) set by the Centers for Medicare and Medicaid Services (CMS) and updated annually in the MPFS. Initially, Medicare based prices for Part B medical services on historical “customary, prevailing and reasonable” charges, a system that led to rapid price inflation. Since 1992, Medicare has employed a system called the Resource-Based Relative Value Scale (RBRVS), which assigns relative values based on resource costs; this approach was meant to be a more objective way to price physician services. CMS decides what services will be covered and sets a reimbursement rate for more than 10,000 services, each of which receives a current procedural terminology (CPT) code. The CPT coding system was created by the American Medical Association (AMA) in 1966 as a standardized way to describe healthcare services in medical records, insurance claims, and research. The AMA maintains copyright ownership of the CPT coding guidelines, and users of the system are generally required to pay a licensing fee.
The RUC
The RUC is a group of 32 physicians, 22 of which are appointed by major national medical-specialty societies. The AMA’s Board of Trustees selects both the RUC chair and the association’s representative to the RUC. Specialty societies nominate RUC individual members, but the AMA must approve them. The RUC was formed by the AMA in 1991 to act as an expert panel in making recommendations to CMS on the relative values of CPT codes, using the RBRVS. The RUC meets three times a year to suggest new services to add to the MPFS and to recommend updates to the relative value units (RVUs) of existing CPT codes. The specialty societies survey their members regarding physician work (PW), practice expense (PE), and professional liability insurance, and the results are presented at the triannual RUC meetings. The RUC then sends its recommendations for relative values to CMS after each meeting. Between 1993 and 2022, the RUC submitted more than 7,400 relative-value recommendations to CMS for new, revised, and potentially misvalued codes, and CMS typically accepts over 90 percent of the recommendations it receives each year.
Assigning RVUs
CMS uses the RBRVS to assign RVUs to each CPT code on the basis of the same three components in the RUC surveys. First, it considers PW, which accounts for the time a procedure takes, the skill and effort it requires, and the stress experienced by the provider in performing it. Next, it calculates RVUs for PE, which accounts for the cost of medical personnel, equipment, supplies, and overhead. The RVUs for PE are different depending on the site where the procedure is performed; it is higher in a physician’s office and lower at a hospital, since hospitals and other facilities receive certain expense-related payments from Medicare that physicians in an outpatient setting do not receive. Last, CMS assigns RVUs to professional liability insurance (PLI)—that is, medical malpractice insurance. PW accounts for about half of total RVUs and PLI for at most 10 percent. CMS recognizes that resource components vary from place to place. For example, a city like Washington, DC commands higher wages (for physicians, nurses, and other supporting staff), higher office overheads, and higher liability risk than does rural West Virginia. CMS has divided the country into 112 zones; each locality receives a Geographic Practice Cost Index (GPCI) for PW, PE, and PLI. CMS calculates the RVUs for a given code in a given locality by multiplying the RVUs for PW, PE, and PLI by the locality’s GPCIs.
RVUs to Dollars: The Conversion Factor
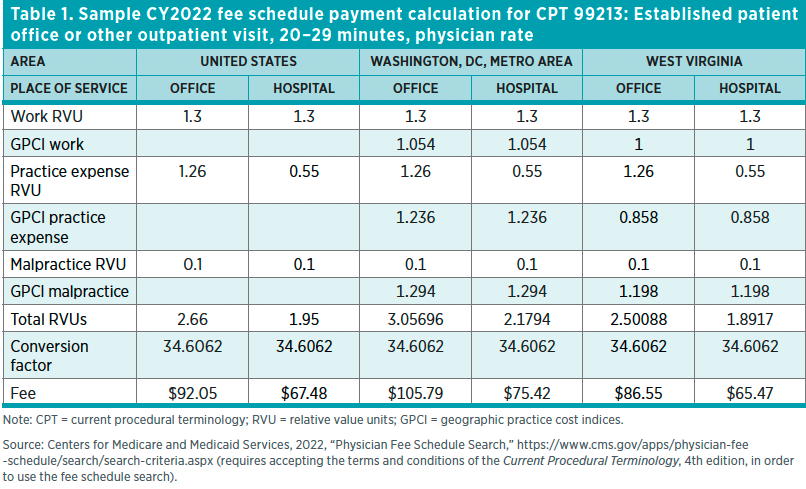
Once each component’s RVUs have been adjusted for locality, the final step is to convert the RVUs into a corresponding reimbursement rate. CMS does this by assigning a dollar value for one RVU. This conversion factor (CF) is updated annually. The number of RVUs is then multiplied by the CF to arrive at a payment amount for each service. In summary, the RVU calculation formula for a given CPT code reads as follows:
[(PW RVU × PW GPCI) + (PE RVU × PE GPCI) + (PLI RVU × PLI GPCI)] × CF = MPFS payment
The resulting number is the locality-adjusted maximum allowable amount, or the maximum price that Medicare will reimburse a provider for providing that particular service to a Medicare Part B enrollee. Table 1 contains an example of one of the most commonly used CPT codes.
MEDICARE’S INFLUENCE ON PRIVATE PRICES
Although traditional Medicare covers the healthcare services of a little more than 10 percent of the population, policies affecting physician reimbursement in Medicare have an impact on the entire healthcare system. Many private plans use a payment mechanism similar to Medicare and may even use the same billing codes. However, studies have found that private insurers’ payment rates are consistently and increasingly higher on average than those of Part B, and when CMS increases or lowers reimbursement rates for Part B, private insurers generally follow suit. The Medicare Payment Advisory Commission (MedPAC) found that, in 2019, private insurance payment rates for clinician services were 136 percent of traditional Medicare’s rates, up slightly from 135 percent in 2018, with certain services marked up more significantly than others. For example, private insurance rates were 128 percent of Medicare rates for evaluation and management (E/M) office visits for established patients but 168 percent of Medicare rates for coronary artery bypass graft surgery.
EFFECTS OF CHANGES TO MEDICARE PRICES ON ACCESS TO CARE
Given the disparity between Medicare and commercial prices, some policy proposals aim to cut healthcare costs by bringing private prices closer to Medicare rates through rate caps, a cap-and-floor policy (setting a range within which commercial prices may fall), or rate setting. However, if private insurers follow Medicare’s lead, another potential solution emerges: CMS could decide to cut Medicare rates. In fact, research shows that when Medicare rates go down, private insurance rates go down as well. A $1 decrease in Medicare’s fees is associated with a $1.30 decrease in private prices. Conversely, a $1 increase in Medicare’s fees is associated with a $1.16 increase in private prices. This relationship between Medicare and private prices is stronger in concentrated insurer markets and competitive physician markets.
One explanation for why providers are willing to accept lower prices from private payers when Medicare rates go down, as opposed to negotiating higher prices to compensate for the losses, is that they increase the volume of care provided to privately insured patients to make up for the lost income. As a result, cutting Medicare rates to achieve lower private rates and lower healthcare spending overall could have unintended consequences, as it may reduce Medicare beneficiaries’ access to care. It would then seem that reimbursement rates can never go down without negatively impacting beneficiaries’ access to care. But MPFS rates do in fact go down. To understand why, we take a closer look at the complex way CMS sets rates and the basic flaws of administrative pricing.
DRAWBACKS OF RBRVS AND THE MPFS PRICING SYSTEM
While it is CMS that issues the MPFS every year, it does not perform the bulk of the work involved in setting the rates. CMS accepts the vast majority of the RUC’s recommendations and does not maintain its own data with which to validate those recommendations. In addition, the US Government Accountability Office (GAO) and others have questioned the accuracy of the RUC estimates and have pointed out the potential conflict of interest inherent in having physicians set the reimbursement rates for physician services. The members of the RUC have little incentive to identify overvalued CPT codes, as doing so would result in cuts to those reimbursements. The RUC is responsible for collecting surveys from peers to inform its recommendations, but GAO identified significant flaws in those surveys: They do not target a representative and random sample of specialists; there is no process to ensure that the specialists weighing in on RVUs for new procedures are familiar with those procedures; expert panels can override survey results (which negates the legitimacy of the surveys that do end up informing the RUC’s recommendations to CMS); PE estimates are based on unrealistic expectations regarding utilization rates and the cost of investment in new equipment; and the best-funded specialties’ lobbying groups have significant influence on the survey process. All these factors create a favorable climate for price-increase proposals.
However, the RUC does not have the ability to push prices up to whatever level its members wish, because Part B is subject to a budget-neutrality rule, meaning that any changes to the MPFS that result in an increase or decrease in Medicare Part B outlays exceeding $20 million will trigger automatic adjustments. Consequently, if the RUC recommends payment increases for certain services, it is forced to recommend cuts for other services. A long-standing problem stemming from the budget-neutrality rule is that it encourages the RUC to propose cuts on relatively low-priced, high-volume services, namely E/M codes that broadly apply to all physician visits and services intended to evaluate and manage a patient’s health. Although E/M services are billed by all physicians, they constitute a larger share of primary care physicians’ bills, because specialists perform procedures more frequently than primary care doctors do. Conversely, procedure-code rates are easier to increase, because they are billed less often than E/M codes and increasing them is less likely to cause Medicare spending to balloon out of control. In addition, most of the members of the RUC are specialists, and just a handful are primary care physicians; this has been cited as a factor that may contribute to procedure-code rate increases. Analyses have shown that Medicare reimburses physicians three to five times more for common procedural care than for E/M care, and some have warned that this could exacerbate the current shortage of primary care providers.
Payment cuts are generally reflected through the RVUs for PW and ultimately the CF. In calendar year (CY) 2023, the CF announced in the MPFS final rule was $33.067, down from $34.6062 in 2022.21 The proposed cut was met with considerable opposition from physician groups, which warned that it threatened the financial stability of practices in the face of soaring inflation and growing rates of physician burnout. Congress subsequently passed the Consolidated Appropriations Act of 2023, which mitigated the cuts set to begin on January 1, 2023. Consequently, CMS announced on January 5, 2023, that the conversion factor would be $33.8872 in CY 2023, a reduction of $0.72 from the CY 2022 rate.
The MPFS is based on an FFS payment mechanism that reimburses physicians for the more than 10,000 individual services in the CPT set. Therefore, if there is no code, there is no billing—and if there is no billing, physicians have no incentive to provide the care. Consequently, Medicare’s administrative pricing undermines innovation in the practice of medicine, because there is likewise no incentive to coordinate care, even when such coordination would be more efficient and would lead to higher quality health outcomes. The necessity for each procedure to be reimbursable by Medicare also encourages innovators to prioritize the development of products and services that Medicare will agree to add to the MPFS. This administrative payment system also offers no incentive for providers to compete based on the quality of their care.
TRANSITION TO VALUE
A basic flaw of the RBRVS is that it bases payment rates on the input costs to provide the service without accounting for the output (i.e., the value of the service to the patient). In 2015, Congress passed the Medicare Access and CHIP Reauthorization Act (MACRA) on a bipartisan basis to address some of the flaws of the RBRVS and to transition providers into innovative alternatives to traditional FFS. Those alternatives are generally referred to as alternative payment models (APMs). Through its Quality Payment Program, MACRA established two payment tracks: the Merit-based Incentive Payment System (MIPS) and the Advanced APM track. MIPS adjusts payment to providers on the basis of performance, which incorporates several things—the quality of care, the way in which electronic health records are used to promote care coordination, activities to improve patient engagement and access to care, and the cost of care. MIPS was originally designed to make FFS increasingly less attractive to providers, encouraging them to participate in APMs. As the name implies, APMs are healthcare payment and delivery models that move away from FFS and toward more aggregated payments. Common examples are Accountable Care Organizations (ACOs), which pay for healthcare services for a defined population of beneficiaries, and bundled payments, which pay for a discrete episode of care. Although APMs represent an opportunity to shift away from FFS, in their current design the relatively few CMS-approved models either have failed to produce substantial savings for the Medicare program or have come with significant financial risk to providers, making them difficult to adopt.
IMPLICATIONS FOR POLICY MAKING
Three decades after the implementation of the MPFS, most policy experts agree that fee schedules and the FFS payment method have led to higher costs by rewarding providers for the volume of services provided, rather than incentivizing them to compete on the value of those services. The ultimate goal of payment reform is therefore to move providers into APMs that aggregate payments and hold providers responsible for the quality and cost of care. However, because fee schedules are currently an inherent part of public and private payment systems, the move away from FFS will not be quick or easy. Although CMS has expressed a commitment to value-based care through innovative payment and delivery models, only six out of more than 50 models launched by the CMS Innovation Center between 2010 and 2020 generated statistically significant savings for Medicare, and the center plans to reduce the number of models it oversees in the coming decade. In addition, the few models that have shown promise still rely heavily on FFS as part of their payment infrastructure.
Policymakers need to take a two-pronged approach to Medicare payment reform. First of all, a budget-neutral rebalancing of the MPFS, achieved by increasing certain rates and lowering others, is needed in order to achieve specific policy goals. At the same time, the potential of Medicare Advantage to increase value and accelerate the transition away from FFS into value-based APMs should be exploited by making Medicare Advantage the default enrollment option for new beneficiaries while making the Medicare Advantage bidding process more competitive.
Fixing the MPFS
Given the likelihood of a protracted transition away from FFS, a number of policies have been offered that could improve the transparency and accuracy of the MPFS process. MedPAC has expressed concern about the accuracy of the data used to set RVUs and has warned that wrong pricing could affect beneficiary access to services and may even contribute to shortages of physicians in primary care specialties that tend to provide a large share of E/M services. In 2018, MedPAC recommended a budget-neutral rebalancing of the MPFS by increasing payment rates for ambulatory E/M services while reducing payment rates for other services, such as procedures, imaging, and tests. Noting that “cost-based payment levels, even if accurately determined, do not necessarily produce a service mix that reflects the desires of beneficiaries,” Urban Institute fellow Robert Berenson and USC Schaeffer Center fellow Paul Ginsburg have suggested that CMS use a broader array of relevant information than is available to it from the current RUC reviews to reevaluate the RVUs for certain codes. This information should go beyond cost-based RVUs to include more accurate estimates of the benefit to patients of services being evaluated, along with an assessment of the impact on access to care from any reduction in fees. They have also suggested that changes to the fee schedule should be targeted to achieve explicit policy aims, such as addressing workforce inadequacies, and should also be complementary to, rather than separate from, value-based policy goals. We propose that Congress give CMS the authority to adopt these policy recommendations as part of a fundamental restructuring of the MPFS that reflects the true value of services based on the needs of beneficiaries.
Although these policy options could serve to make the MPFS more accurately reflect the cost of providing services in the near term, they do not address the current shortage of viable APMs. More APMs are needed to achieve the long-term goal of moving Medicare away from FFS and administrative pricing to a truly value-based payment system.
Medicare Advantage as an APM
Medicare beneficiaries can choose whether to receive their benefits from a traditional Medicare plan or a Medicare Advantage plan offered by private insurers. Enrollment in Medicare Advantage more than doubled between 2010 and 2020, and by 2025 it is expected that 50 percent of Medicare beneficiaries will be enrolled in Medicare Advantage. Unlike traditional Medicare, which pays for individual services provided to a beneficiary, in Medicare Advantage the federal government pays private insurers a fixed amount per beneficiary, adjusted for medical complexity, to provide the services covered under traditional Medicare; most plans offer additional benefits without additional costs to beneficiaries or taxpayers. Currently, CMS administratively sets county-level benchmarks—that is, the maximum monthly prospective per-beneficiary amount that plans can receive as a share of per capita traditional Medicare spending. Based on historical spending in traditional Medicare in each county and adjusted for demographics, the resulting benchmarks are inversely proportional to the county-level traditional Medicare spending. Benchmarks are also adjusted on the basis of quality, with plans that have a higher quality rating receiving an upward adjustment.
Plans then offer bids to cover enrollees’ health benefits. If the bid is above the benchmark, the plan can charge the beneficiary an additional premium. If the plan bid is below the benchmark, the beneficiary pays no additional premium, and a percentage of the difference between the benchmark and the bid is returned to the plan as a rebate, to be used to provide additional benefits, reduce costs to the beneficiary, or invest in care-delivery improvements. If the plan is unable to control costs to the level anticipated, the additional costs are the responsibility of the plan, not of Medicare and the taxpayer.
Although there is an ongoing debate about whether Medicare Advantage plans are overpaid, there is evidence that Medicare Advantage has the potential of providing comprehensive, high-quality, low-cost care to beneficiaries. According to a Kaiser Family Foundation analysis, in 2022 most enrollees in Medicare Advantage were in plans that provided access to benefits not covered by traditional Medicare, including eye exams, glasses, or both (99 percent); hearing exams, aids, or both (98 percent); telehealth services (98 percent); dental care (96 percent); and a fitness benefit (98 percent). The vast majority of Medicare Advantage enrollees paid no supplemental premium (other than the Part B premium) in 2022, and Medicare Advantage premiums that include prescription-drug coverage have steadily declined since 2015. Medicare Advantage has been shown to result in large reductions in institutional (Part A) utilization and spending when compared to traditional Medicare; this is due in large part to greater use of screening and preventive services and a reduction in hospital admissions. Medicare Advantage has also been shown to equal or outperform traditional Medicare on a number of quality measures, including a reversal of the racial and ethnic disparities in mammography screening seen in traditional Medicare and improved access to care for adults with low income.
As a capitated, population-based payment model, Medicare Advantage represents the ideal in an APM. In addition, private plans in Medicare Advantage are more flexible and innovative than in traditional Medicare. According to the Health Care Payment Learning and Action Network, in 2020 a significantly greater percentage of Medicare Advantage payments flowed through more advanced category 3 and 4 payment models compared to traditional Medicare. In 2018, CMS announced the Medicare Advantage Qualifying Payment Arrangement Incentive Demonstration to test whether incorporating certain payment arrangements within Medicare Advantage organizations into MACRA would increase participation in payment arrangements similar to Advanced APMs and change the manner in which clinicians deliver care. However, CMS discontinued the demonstration in 2019, citing low participation.
Johns Hopkins University assistant professor Brian Miller and former CMS administrator Gail Wilensky have proposed changing the default enrollment for new Medicare beneficiaries from traditional Medicare to Medicare Advantage. Under this proposal, if new beneficiaries did not select a Medicare Advantage plan or elect FFS Medicare, they would be automatically assigned to a Medicare Advantage plan with a star quality rating of 3.5 or higher and would retain the option of disenrolling into FFS during the existing standard annual disenrollment period. A number of states already use Section 1115 demonstration or Section 1915 waiver authority to employ autoenrollment with their Medicaid and dual-eligible populations. In order to utilize the full potential of Medicare Advantage to accelerate the transition to value-based care, Congress and the Secretary of Health and Human Services should carry out the necessary legislative and regulatory changes in order to establish Medicare Advantage as the default enrollment option for all new Medicare beneficiaries.
Similar to administrative pricing in the MPFS, administrative determination of benchmarks in Medicare Advantage is considered by many to be problematic. For example, the Office of the Assistant Secretary for Planning and Evaluation has expressed concern that changes in Medicare Advantage benchmark calculations authorized by the Affordable Care Act—changes meant to reduce payments to Medicare Advantage plans—may not provide the incentives for value and innovation that could be realized by a fully competitive program. Proposals to increase competition and reduce costs in Medicare Advantage have included abandoning the current system of setting benchmarks in favor of a truly competitive bidding system that would either be limited to Medicare Advantage plans or include traditional Medicare in the bidding process. Policymakers should abandon administratively set pricing and allow for truly competitive bidding in the establishment of benchmarks in the Medicare Advantage program as proposed by Chakravarthy, Wilensky, and Miller. A substantial change to payment policy in Medicare Advantage will encounter political and implementation challenges and will likely need to be phased in to mitigate program disruption. However, basing the benchmarks on the distribution of bids rather than on an administratively determined level would help to relieve Medicare of its role in setting prices and would provide stronger incentives for plans to increase the value of services delivered.
CONCLUSION
As the nation’s largest healthcare payer, accounting for more than one in five dollars spent on healthcare within the United States, Medicare has a substantial impact on US healthcare spending. To pay for Part B services, Medicare decides which services will be covered and sets relative values for more than 10,000 individual services, using data of suspect accuracy. The amount Medicare will pay for each service is published in the MPFS, which is developed, maintained, and updated annually by the CMS. This administrative pricing system, based on FFS and RBRVS, rewards volume over the value of services and contributes to growth in healthcare spending.
The ultimate goal of payment reform is to move away from FFS and administrative pricing to payment models that allow providers to compete on the basis of the value of their care. However, since FFS is an entrenched part of public and private payment infrastructure, policies are needed that will improve the accuracy of the data used to price Part B services, at least in the short term. In addition, policymakers should make Medicare Advantage the default enrollment option for new Medicare beneficiaries and introduce genuine competition in Medicare Advantage to fully utilize the potential of the program to accelerate the transition to APMs and value-based healthcare.
ABOUT THE AUTHORS
John O’Shea is a surgeon and a senior fellow at the Texas Public Policy Foundation. Previously, he was a senior fellow at the Heritage Foundation, visiting scholar at the Brookings Institution, and senior policy advisor for the US House of Representatives, Committee on Energy and Commerce.
Elise Amez-Droz is a program manager for the Open Health project at the Mercatus Center at George Mason University.
Kofi Ampaabeng is a research fellow and data scientist at the Mercatus Center at George Mason University. He specializes in curating data and generating policy-relevant insights from data. Before joining the Mercatus Center, he worked for IMPAQ International, LLC, where he evaluated the efficacy of government programs.
Citations and endnotes are not included in the web version of this product. For complete citations and endnotes, please refer to the downloadable PDF at the top of the webpage.

