- | Healthcare Healthcare
- | Policy Briefs Policy Briefs
- |
Raising the Bar: ICU Beds and Certificates of Need
The nation is on a mission to “flatten the curve.” The goal is not so much to reduce the total number of COVID-19 infections—though that would be ideal—but to reduce the number of infections at any one time, so as to ensure that the nation’s healthcare resources are not overwhelmed. While it has received less attention, a secondary goal should be to “raise the bar” by increasing the nation’s capacity to handle those cases that do arise (see figure 1). Certificate-of-need (CON) laws may contribute to diminished healthcare capacity, and their elimination can help raise the bar so that the nation is ready for the next healthcare crisis.
In the next section, we briefly describe CON laws and their relationship with cost, quality, and access. In section II, we use intensive care unit (ICU) bed shortage projections to examine how CON regulation of hospital beds relates to shortages. We find that those states that require a CON for hospital beds are more than twice as likely to experience projected ICU bed shortages. On average, these states are expected to experience an ICU bed shortage of about 8,000 beds (about 9 beds per 10,000 residents). By contrast, states that do not require a CON for hospital beds are expected to experience an average shortage of about 114 ICU beds (about 1 bed per 10,000 residents). We also find that the temporary suspension of CON has no statistically significant relationship to ICU bed shortages.

I. A Brief Introduction to Certificate-of-Need Laws
In 35 states and the District of Columbia, healthcare providers must obtain permission from a regulator before they may open new facilities, expand existing ones, or acquire new equipment. These CON requirements vary from state to state and cover a variety of services and equipment, including new or expanded hospitals, hospital beds, medical imaging technologies, drug rehabilitation centers, mental health facilities, and neonatal ICUs. Unlike other varieties of regulation, CON is not intended to assess a provider’s qualifications, credentials, or safety record. Instead, CON charges regulators with assessing the provider’s claim that the medical service is actually needed.
Controversially, the CON approval process invites incumbent providers to challenge the applications of their would-be competitors. And even if a CON is granted, applicants can expect the process to take months or even years, and it has been known to cost providers hundreds of thousands of dollars.
Peer-reviewed academic studies have found that CON laws are associated with higher costs and lower-quality care. But by far the most studied aspect of CON laws is their effect on healthcare capacity. In careful studies that control for possibly confounding effects, researchers find that CON laws are associated with
- fewer hospitals per capita;
- fewer ambulatory surgical centers per capita;
- fewer rural hospitals per capita;
- fewer rural ambulatory surgical centers per capita;
- fewer hospital beds per capita;
- fewer hospice care facilities;
- fewer dialysis clinics;
- fewer hospitals offering MRI, CT, and PET scans;
- longer driving distances to obtain care; and
- greater racial disparities in the provision of care.
The estimated size of these relationships is often quite large. One study, for example, found that CON states have 30 percent fewer hospitals per capita than non-CON states. Another found that, compared with non-CON states, in states where a CON is required to obtain a hospital bed, there are 13.1 fewer hospital beds per 10,000 residents.
Hospital beds are a particularly important aspect of healthcare capacity in the fight against COVID-19. As shown in figure 2, 27 states require providers to obtain CONs before acquiring hospital beds. In many cases, providers must obtain CONs even to relocate beds from one facility to another. In the next section, we examine how these rules relate to bed shortages.

II. Estimated ICU Bed Shortages
The Institute for Health Metrics and Evaluation (IHME) has produced a number of widely cited estimates of hospital capacity shortages in light of COVID-19. For each state, it has estimated lower-bound, upper-bound, and mean ICU bed shortages over the first seven months of 2020. Figure 3 shows national estimates (as of April 22) of ICU bed shortages. One can think of these as the portions of the curve in figure 1 that lie above the horizonal capacity line.
According to IHME’s mean estimate, the national ICU bed shortage peaked on April 14 at about 9,000 beds. According to the worst-case scenario, the ICU bed shortage will peak later in April at about 23,000 beds.
According to these estimates, however, the ICU bed shortage is driven mostly by a few states. In most states, there will be no shortage at all. This is some indication that the public’s precautionary measures are flattening the curve. It also reflects the fact that most hospitals have been ordered to cancel elective procedures, freeing up resources for COVID patients. As many have noted, however, this strategy is not sustainable. Hospitals are postponing needed procedures such as mastectomies and chemotherapy treatments for less aggressive cancers. And because elective procedures are their bread and butter, hospitals are hemorrhaging money that will be necessary to pay those caregivers who are on the frontlines fighting COVID. The financial viability of these hospitals will be especially important if the virus returns in the fall.

III. ICU Bed Shortages and Certificates of Need
Figure 4 shows those states in which the IHME’s mean estimate projects an ICU bed shortage. Eleven states in total are expected to experience a shortage of ICU beds; eight of these require a CON for hospital beds.

Figure 5 shows the share of states that are projected to experience an ICU bed shortage, broken down by whether or not the states require a CON for hospital beds. Among those states that do not require a CON for hospital beds, 13 percent are projected to experience a shortage, according to the mean estimate. But among those states that require a CON for hospital beds, 30 percent are projected to experience an ICU bed shortage. The difference between these sample means is statistically significant at the 10 percent level.



IV. Discussion
According to our analysis, states that require a CON for hospital beds are statistically significantly more likely to experience a shortage of ICU beds over the course of the COVID-19 pandemic. The shortages are expected to be larger in these states, both in absolute and in per capita terms. To be precise, there is a 13 percent chance that the average non-CON state will experience a shortage of ICU beds, while there is a 30 percent chance that the average CON state will experience such a shortage. The average non-CON state is expected to experience a shortage of 114 ICU beds (a little more than 0.5 beds per 10,000 residents) over the course of the pandemic, while the average CON state is expected to experience a shortage of over 8,000 beds (about 9 beds per 10,000 residents) over the course of the pandemic.
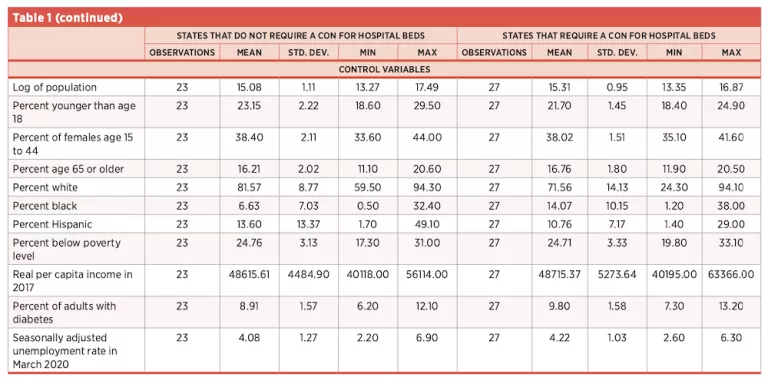
To see if these differences were possibly driven by confounding factors, we gathered state demographic data on race, gender, age, economic conditions, and underlying health factors. Table 1 shows the descriptive statistics for these factors, broken down by whether or not states require a CON for hospitals beds. In most cases, these factors do not differ between CON and non-CON states. There are, however, statistically significantly more black individuals and more adults with diabetes in CON states relative to non-CON states. The differences in ICU bed shortages between CON and non-CON states, however, remain statistically significant in regression models that control for these factors.
So far, 22 states have temporarily suspended or somehow relaxed their CON requirements to make it easier for providers to increase capacity. We ran tests to see if these temporary policy changes made a difference in terms of shortages and found that they have no statistically significant relationship with ICU bed shortages. This suggests that it may take weeks or perhaps even months to build this capacity.
Overall, the results suggest that CON regulators have not accurately assessed the public’s need for ICU beds in the event of a potentially catastrophic pandemic. Policymakers who wish to “raise the bar” so that their states are better prepared to face the next health crisis should consider eliminating their CON laws.




About the Authors
Matthew D. Mitchell is a senior research fellow and director of the Equity Initiative at the Mercatus Center at George Mason University. He is also an adjunct professor of economics at George Mason University. In his writing and research, he specializes in public choice economics and the economics of government favoritism toward particular businesses, industries, and occupations.
Thomas Stratmann is a senior research fellow at the Mercatus Center and professor of economics and law at George Mason University. His primary research interests are political economy, fiscal policy, law and economics, health economics, and experimental economics.
James Bailey is an assistant professor of economics at Providence College, a visiting scholar at the Federal Reserve Bank of Philadelphia, and a senior affiliated scholar with the Mercatus Center at George Mason University. He previously taught at Creighton University and the University of West Florida. He earned a PhD in Economics and a master’s in Economics from Temple University.

