This Mercatus on Policy examines how the low quality of both the ACA regulations and the Bush administration’s early homeland security regulations highlight the need for reforms to strengthen the quality of regulatory analysis.
What do the Obama administration’s first few major health care regulations and the Bush administration’s first few major homeland security regulations have in common? Both reflected a president’s signature high-priority issue. Both took the form of “interim final rules” issued under tight legislative deadlines. Both exemplify “fire, ready, aim” rulemaking at its worst. And both were accompanied by low-quality regulatory analysis that reads more like an attempt to justify decisions than an attempt to inform decisions.
When the White House directs agencies in fast-tracked rulemakings, many of the usual checks that should ensure that good analysis informs decisions get short-circuited. Regulatory process reforms would prevent this problem.
The Systemic Problem
Executive Order 12866 requires federal agencies to produce regulatory impact analyses (RIAs) when they propose regulations. The analysis requirements are most comprehensive for the most important regulations: those termed “economically significant.” When proposing a regulation, an agency must assess the systemic problem the regulation is supposed to solve, define the outcomes the regulation is supposed to produce for the public, examine a wide variety of alternative solutions, and assess the pros and cons (benefits and costs) of the alternatives. The agency must publish the RIA along with the proposed regulation for public comment, and the agency must consider the comments when they write the final version of the regulation.
Many of the first health care and homeland security regulations, however, were interim final rules. This means the agencies decided on, wrote, and published the rules without first publishing a proposal or RIA for public comment. The Department of Health and Human Services (HHS) and other agencies published eight economically significant interim final rules implementing the Patient Protection and Affordable Care Act (ACA) in 2010. The Department of Homeland Security (DHS) published seven economically significant interim final rules between 2003 and 2007.
The RIAs accompanying both sets of regulations were seriously incomplete, and they fell far short of federal agencies’ normal practice.

Incomplete Regulatory Analysis
The health care RIAs presented no monetary estimates of benefits, often overestimated the number of people who would benefit, and usually underestimated costs, often by hundreds of millions or billions of dollars. Despite the importance of fairness and equity in the health care debate, analysis of equity was even more superficial—usually consisting of mere assertions that some result would improve “equity” without even defining the term.
The Bush administration’s early homeland security regulations tended to overestimate benefits and underestimate costs. They rarely identified the systemic problem the regulation was supposed to fix or evaluated alternatives to the proposed regulation. Nor did they explain why federal action was necessary to safeguard facilities and assets where the private sector had substantial investments at stake.
Analysis Fails to Meet Normal Standards
The Mercatus Regulatory Report Card evaluates the quality and use of regulatory analysis based on criteria derived from Executive Order 12866 and Office of Management and Budget (OMB) guidance. Report Card criteria fall into three categories: Openness (how accessible, clear, and well documented is the analysis?); Analysis (how well does the analysis identify the desired outcomes, systemic problem, alternatives, costs, and benefits?); and Use (to what extent did the agency claim to use the analysis or make provisions for retrospective analysis of the regulation?). A regulation can earn a maximum of 20 points for each category.
Figure 1 compares the quality and use of analysis for six prescriptive interim final ACA regulations with that for economically significant regulations proposed by all agencies and by HHS in 2008 and 2009:
- The ACA regulations perform best on the openness criteria. These are the easiest criteria to do well on.
- The ACA regulations fare poorly on the analysis criteria, earning fewer than half the possible points.
- The ACA regulations score much worse than other regulations on the use criteria with virtually no evidence that
- the departments used the analysis to make decisions
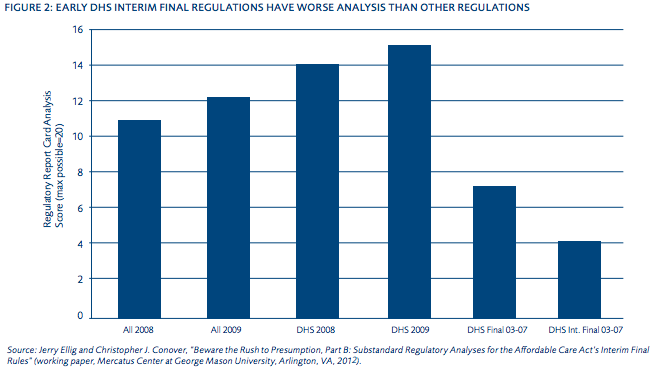
A pilot study that preceded the Regulatory Report Card assessed DHS regulations according to the four analysis criteria. Figure 2 compares the six prescriptive interim final rules issued by DHS during its first few years with other regulations. The interim final DHS regulations earned only onequarter of the possible points for quality of analysis—well below the quality of other federal regulations, recent DHS regulations, and regulations issued by DHS in its first five years that were not interim final regulations.
The ACA and DHS interim final regulations earned similar scores for quality of analysis. The analysis falls far short of the analyses normally conducted, which generally falls well below the standards outlined in Executive Order 12866 and OMB’s Circular A-4.
 The Root Causes
The Root Causes
The ACA rules analyzed encompassed nearly all the major components of the ACA scheduled to go into effect prior to 2014. Congress gave the agencies deadlines that ensured the regulations would be written before control of Congress changed hands after the 2010 elections and implemented before the 2012 elections. Similarly, Congress explicitly told DHS to issue five of the homeland security rules as soon as practicable as interim final rules.
Health care and homeland security are the signature initiatives of the Obama and Bush administrations, respectively. In her classic 2001 Harvard Law Review article on “Presidential Administration,” Elena Kagan revealed how the Clinton White House proactively set the regulatory agenda for agencies and directed development of high-priority regulations. She predicted future presidents would continue this practice, and subsequent scholarship has proven her prediction accurate.
At least for some presidential regulatory priorities, many key decisions are already made before the regulatory analysis is done. Thus, it is unlikely agency analysts will put much effort into the analysis, as it will have little effect on decisions. It is also unlikely that OMB’s Office of Information and Regulatory Affairs (OIRA) could block the regulation, so OIRA has little leverage to prompt improvements in the analysis.
Consistent with this hypothesis, the interim final health care regulations received rapid review at OIRA, averaging just five days. The DHS rules received somewhat longer review, averaging 22 days. By comparison, OIRA took an average of 27 days to review proposed economically significant regulations in 2009 and 56 days in 2008.
The poor quality and use of analysis for these regulations is an institutional problem that requires an institutional solution. Both the Bush and the Obama administrations pledged to improve the quality of regulatory analysis. Both appointed noted regulatory scholars as OIRA administrators—John Graham and Susan Dudley in the Bush administration and Cass Sunstein in the Obama administration. The Bush administration published an updated, extensive, peer-reviewed guidance for regulatory analysis (Circular A-4) and sought to rein in “midnight regulations.” The Obama administration issued a memorandum urging departments to respect scientific integrity, sought public comments on revising Executive Order 12866, and ultimately reaffirmed it with Executive Order 13563. Deficiencies in the quality and use of analysis occurred despite these good intentions.
Regulatory Reform Solutions
Alternative checks are needed to insulate analysis from presidential and congressional politics:
- Require agencies to publish an assessment of the systemic problem, its root cause, and the pros and cons of alternative solutions for public comment before writing a proposed rule. The public would have an opportunity to replicate, improve, or comment upon the agency’s analysis before it is used to make decisions.
- Designate an independent authority to review RIAs produced by the executive branch. Such review could be competently performed in a nonpartisan manner by the Congressional Budget Office or Government Accountability Office, provided that they are clearly empowered and staffed to conduct an objective review.
- Mandate external peer review with systematic monitoring. Without systematic monitoring by OIRA or Congress (e.g., random audits of RIAs), there may be little incentive for agency staff to incorporate the suggestions of peer reviewers.
- Explicitly rein in the use of interim final rulemaking. In principle, an agency can amend an interim final rule based on public comments, but this happens less frequently than for rules issued under the normal process. 12 Interim final rules should be reserved for genuine emergencies or routine, uncontroversial administrative decisions.
To read the other papers in this study, please see: "Beware the Rush to Presumption: Regulatory Analysis and the Affordable Care Act's Interim Final Rules."

