- | Healthcare Healthcare
- | Policy Briefs Policy Briefs
- |
Telehealth Payment Parity Laws at the State Level
During the coronavirus pandemic, the use of telehealth—especially real-time video conferencing to provide medical care—has sharply increased. State governments and the federal government have made several policy changes to facilitate access to telehealth in general and telemedicine in particular, such as granting waivers to insurers and regulators for telemedicine regulations and mandating that private insurance plans cover telemedicine if they cover the same services when those services are provided in person. The latter policy change especially has rapidly expanded the prevalence of state-level telemedicine parity laws that apply to private health insurance plans.
Since 1995, 40 states and the District of Columbia have implemented telemedicine coverage parity mandates, which require private insurance plans that comply with the Employee Retirement Income Security Act cover a telemedicine service if they also cover the same service when it is provided face-to-face. Those laws expanded the use of telemedicine. In some states, the mandates went further and mandated payment parity. Payment parity mandates require parity for covered telemedicine service in reimbursements, coverage, or both compared with equivalent in-person services. The Coronavirus Aid, Relief, and Economic Security (CARES) Act also includes a payment parity requirement for Medicare, and many private insurers have followed this example by ensuring payment parity for telemedicine.
Advocates for payment parity argue that telemedicine visits are costly to set up and consume the same amount of resources—or more—as in-person visits. Payment parity laws provide resources for providers to cover these costs. Opponents insist that telemedicine lowers healthcare costs, so payment parity mandates act like price controls and encourage overconsumption of healthcare services. But the surge of telemedicine authorizations and parity mandates that has occurred during the pandemic may end before the debate on the merits of parity is settled, because in many states, telemedicine parity mandates will automatically sunset or will expire when the state of emergency that created them expires.
In this policy brief, I review the existing evidence on telemedicine parity mandates. I also discuss how payment parity mandates likely differ from coverage parity mandates and suggest alternatives to payment parity mandates.
Telemedicine before the Pandemic
Telemedicine includes several services and technologies, such as real-time video conferencing, electronically transmitting medical images to specialists, remote patient monitoring, and mobile health apps. Healthcare providers use telemedicine to treat a variety of conditions. For example, real-time video conferencing connects patients with behavioral health conditions to specialists in another location; radiologists, pathologists, dermatologists, or ophthalmologists can review images sent electronically by nonspecialists; data from blood sugar monitors or implanted cardiac devices are sent directly to providers for review; and patients use mobile health apps to track their diet and symptoms. Telemedicine has great potential for treating mental health disorders, ischemic heart disease, cerebrovascular diseases, and diabetes.
Figure 1 shows the states with telemedicine coverage parity mandates and the states with both coverage and payment parity mandates. The 10 states without a mandate are Alabama, Florida, Idaho, North Carolina, Oklahoma, Pennsylvania, South Carolina, Utah, Wisconsin, and Wyoming.
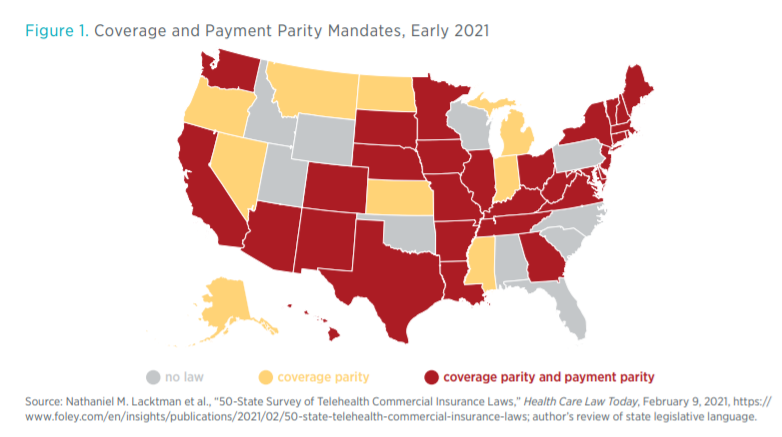
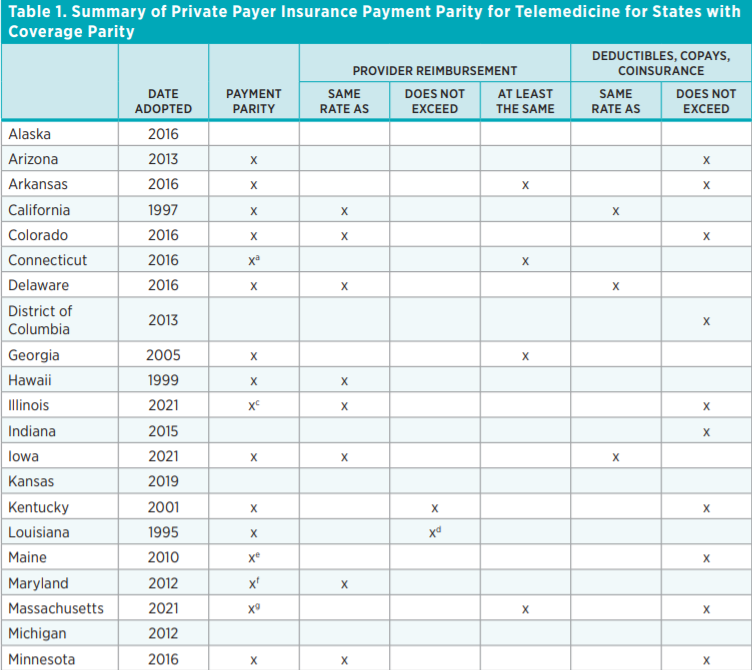
Thirty-one states mandate both coverage parity and a payment parity. Table 1 summarizes the payment parity mandates in states with coverage mandates. The language of the payment parity mandates differs by state. In eight states, the mandated payment applies only to the deductibles, copayments, and coinsurance faced by the insured. For example, in Texas, coinsurance, copayments, and deductibles for telemedicine “may not exceed” those for the same service provided in person. (Some compilations of telemedicine mandates do not refer to such requirements as payment parity mandates because the requirements do not address reimbursement rates for healthcare providers.) Many states mandate parity in how insurance plans reimburse providers. For example, in Arkansas and California, reimbursement for healthcare services provided via telemedicine must be “on the same basis as in person services.” Some payment mandates require “not more than” (5 states), some require “not less than” (6 states), and some require “the same as” (12 states) what is paid when the service is provided face-to-face.

In response to the COVID-19 pandemic, 22 states have implemented emergency policies around private insurance of telemedicine including, for example, mandating coverage of services delivered via telephone. The governors of Colorado, Massachusetts, New York, Ohio, and Texas used emergency executive orders to compel private insurance plans to waive patient cost sharing for telehealth visits during the pandemic. These executive orders last only as long as the declared state of emergency. As the policy ending dates approach, many states are considering whether to maintain these emergency provisions even after the emergency ends.
Effects of Coverage Parity Mandates
Coverage mandates increase the use of telemedicine. This is not surprising, given the findings of extensive research on other kinds of coverage mandates. In healthcare generally, when states mandate coverage of a service, such as fertility treatments or mental health treatments, these mandates increase premiums, reduce the out-of-pocket expense of obtaining the covered service, and increase use of the covered service. In telemedicine specifically, the use of telemedicine increases among those insured by plans covered by the mandates and, as providers invest in the skills and infrastructure needed to provide care via telemedicine, the use of telemedicine increases among those insured by plans not covered by the mandates.
Telemedicine parity mandates do not lower quality of care. A meta-analysis of 93 randomized control trials finds that care provided via telemedicine is of the same or higher quality than in-person care. My own research, conducted with Jiajia “JJ” Chen, demonstrates that state telemedicine parity mandates lower mortality.
Whether telemedicine increases healthcare spending depends on whether telemedicine costs more than in-person care. It also depends on whether telemedicine substitutes for in-person care or increases the amount of (unnecessary) care patients receive overall.
Whether telemedicine is more expensive than equivalent care delivered in person is unclear. A 2015 meta-analysis finds that some, but not all, cost-effectiveness studies show reductions in cost with telemedicine. Physicians at the University of Michigan document that physician-led video visits last a similar amount of time to in-person clinic visits and cost a similar amount of resources; physicians spend more time with the patient during a video visit than during an in-person clinic visit but save money owing to reduced office staff and medical assistant time. A less expensive option is physician assistant–led video visits. Similarly, a time-use study of an orthopedic surgery practice at Penn Medicine finds that the total time, and thus cost, is longer for a telemedicine visit than for an in-person visit. Telemedicine may not be less expensive for medical providers than in-person care unless the change in delivery method also allows for other changes, such as the use of physician assistants.
When a telemedicine visit substitutes for an urgent care or emergency room visit, costs are significantly lower. Furthermore, telemedicine may lower patients’ implicit costs by reducing travel and waiting. Patients, particularly those with chronic conditions requiring regular visits, such as heart disease or diabetes, may prefer the convenience of telemedicine.
Telemedicine coverage mandates may increase the amount of care provided and may increase the amount of telemedicine that substitutes for usual, in-person care. Researchers at Seton Hall University demonstrate that telemedicine coverage mandates increased private insurance enrollment as well as routine checkups; in urban areas, they observe declines in hospital care. These shifts imply a change in the mix of care, likely reducing costs. Whether telemedicine adds to the amount of care patients receive likely depends on its price for patients as well as its costs to providers.
Types and Effects of Payment Parity Mandates
Payment parity mandates come in a variety of forms. Some mandates apply to provider reimbursement, and others apply to patient copayments, coinsurance, and deductibles; many states’ mandates apply to both. Some payment parity mandates require payments to be “on the same basis” as in-person services, and others require payments “not less than” or even “not more than” those for in-person services. The effects of a payment parity mandate depend on its specific language. That said, all payment parity mandates are price controls. Price controls have predictable effects on markets—price ceilings (maximum legal prices) lead to shortages; price floors (minimum legal prices) lead to surpluses. Price controls in healthcare encourage economically inefficient behaviors because providers, insurers, and patients actively seek to avoid the losses and costs that result from regulation.
The impact of price floors on US healthcare markets is complex owing to the prevalence of third-party payment. However, given that healthcare providers argue in favor of payment parity mandates and health insurers argue against them, it is possible that health insurers enjoy an economic rent that may be redistributed to telemedicine providers by mandates.
The prevalence of third-party payers has caused much of the debate on payment parity mandates to revolve around reimbursements. When permitted to negotiate separate rates, reimbursement rates for telemedicine tend to be lower than those for the same service provided in person. For example, one 2014 analysis estimates that a telehealth visit costs $50 for a commercially insured patient, whereas a physician office visit costs $98. This finding implies that reimbursement parity mandates are price floors, artificially setting reimbursement rates higher than market rates. By contrast, reimbursement mandates that require “not more than” in-person rates are price ceilings. These price ceilings are unlikely to affect the market because market participants already agree to telemedicine prices less than those of in-person services.
Payment parity mandates reassure providers that they will be reimbursed for telemedicine. This reassurance likely encourages providers to increase telemedicine visits as well as to invest in needed infrastructure such as technology, staff, different clinical scheduling, and assistance for patients in obtaining and using telemedicine technology.
Health insurers likely do not benefit from payment parity mandates, and they testify against them, arguing that they should be able to negotiate appropriate reimbursement rates for services. Insurers currently negotiate reimbursement rates for newly approved treatments, and some question why telemedicine should be treated differently.
Payment parity mandates also affect patients because these mandates prevent any cost savings from being passed along to patients in the form of lower premiums, deductibles, copayments, or coinsurance. Those savings would otherwise reflect the possibility that care can be provided more efficiently via telemedicine without reducing quality.
Payment parity mandates could have unintended consequences. They could encourage providers to overinvest in infrastructure or to make changes in care provided and billed for. Providers may also tweak telemedicine services to create the appearance of equivalence with well-reimbursed in-person services. Finally, providers may respond to payment parity mandates by billing for services not currently billed for or by shifting too much of their schedule to telemedicine, requiring patients—even those who want in-person services—to access care via telemedicine.
Insurers, in turn, may respond by attempting to discourage telemedicine visits. For example, insurers may cover fewer in-person services that have telemedicine counterparts, or they may negotiate lower rates for in-person services—rates that are too low for the in-person service and too high for telemedicine. Insurers may adjust their in-network list to include providers who agree to lower rates and deliver primarily via telemedicine, shifting patients from their preferred medical professionals.
Mandates for parity in copayments, coinsurance, and deductibles distort patients’ incentives to discriminate between in-person and remote care. Insurers use out-of-pocket costs to encourage enrollees to use cost-effective providers and services, but parity mandates would nullify the ability of insurers to encourage telemedicine over in-person care.
Policy Alternatives
If policymakers want to encourage medical providers to invest in telemedicine infrastructure, there are more efficient ways to achieve this goal than payment parity mandates. Much of the costs of investing in telemedicine are fixed costs: investing in telemedicine carts, changing clinical schedules to allow for both in-person and telemedicine visits, or investing in devices and data analytics to collect and analyze incoming information from remote patient monitoring. Fixed costs imply, at most, a limited period of cost-effectiveness for payment parity mandates. Once investments are paid off, payment parity mandates only encourage overuse of telemedicine services. Sunset provisions denoting the end of payment parity mandates, such as Maryland’s mandate, which is in effect until June 30, 2023, provide a window of “overpaying” to encourage investment. Alternatively, a one-time incentive from insurers for providers to invest in infrastructure would shift care toward telemedicine without distorting incentives in the long term.

