- | Healthcare Healthcare
- | Policy Briefs Policy Briefs
- |
West Virginia’s Certificate-of-Need Program: Lessons from Research
In West Virginia, healthcare providers who wish to open or expand facilities must first obtain a certificate of need (CON). They can acquire this only if they can prove to the satisfaction of the West Virginia Health Care Authority that their community needs the service in question. The purpose of CON regulation is to limit spending by discouraging providers from acquiring unnecessary medical equipment. Unfortunately, in practice, the rules appear to protect incumbent providers from competition more than they protect patients from harm or payers from unnecessary costs.
In this brief, I review the history of CON laws, compare West Virginia’s CON program to the programs in other states, and provide an overview of the economic evidence suggesting that these laws harm patients and taxpayers. I conclude with several reforms—including outright repeal—that could improve outcomes for patients, particularly in low-income and rural areas.
Introduction to CON Laws
CON laws require healthcare providers wishing to open or expand a healthcare facility to first prove to a regulatory body that their community needs the services the facility would provide. The regulations are typically not designed to assess a provider’s qualifications or safety record. Other regulations such as occupational licensing aim to do that. Instead, CON laws aim to determine whether a service is economically viable and valuable.
The process for obtaining a CON can take years and can cost tens or even hundreds of thousands of dollars in preparation costs. Although these regulations appear to benefit incumbent providers by limiting their competition, the regulations’ effects on patients and taxpayers have generally been found to be negative. This finding helps explain why antitrust authorities at the Federal Trade Commission (FTC) and at the US Department of Justice (DOJ) have long taken the position that these rules are anticompetitive. In a joint report from 2004, for example, the FTC and DOJ declared,
The Agencies believe that, on balance, CON programs are not successful in containing health care costs, and that they pose serious anticompetitive risks that usually outweigh their purported economic benefits.
A Brief History of CON Regulation
More than four decades ago, Congress passed and President Gerald Ford signed the National Health Planning and Resources Development Act of 1974. The statute enabled the federal government to withhold federal funds from states that failed to adopt CON regulations in healthcare.
New York had already enacted the first CON program in 1964; by the early 1980s, with the federal government’s encouragement, every state except Louisiana had implemented some version of a CON program. Policymakers hoped that these programs would restrain healthcare costs, increase healthcare quality, and improve access to care for poor and underserved communities.
In 1986—after Medicare changed its reimbursement practices and as evidence mounted that CON laws were failing to achieve their stated goals—Congress repealed the federal act, eliminating federal incentives for states to maintain their CON programs. Since then, 15 states, representing about 40 percent of the US population, have done away with all or most of their healthcare CON regulations, and many others have pared them back. A majority of states still maintain CON programs, however, and vestiges of the National Health Planning and Resources Development Act can be seen in the justifications that regulators and state legislatures offer in support of these regulations.
CON Regulation in West Virginia
West Virginia operates an extensive CON program, requiring providers to obtain permission before making changes to equipment, services, facilities, hospital beds, and nonhospital beds. West Virginia’s CON application fees can be as high as $35,000, though applicants typically spend much more on consulting fees and compliance costs. The application process typically takes 60–105 days, depending on whether a hearing is scheduled. Incumbent providers are allowed to challenge the applications of their would-be competitors.
Table 1 shows the number of technologies and procedures regulated by West Virginia and by the surrounding states. Among all states with CON regulations, the average number of technologies and procedures regulated is 15. In the region surrounding West Virginia, the average is also 15. West Virginia regulates 24 technologies and procedures.
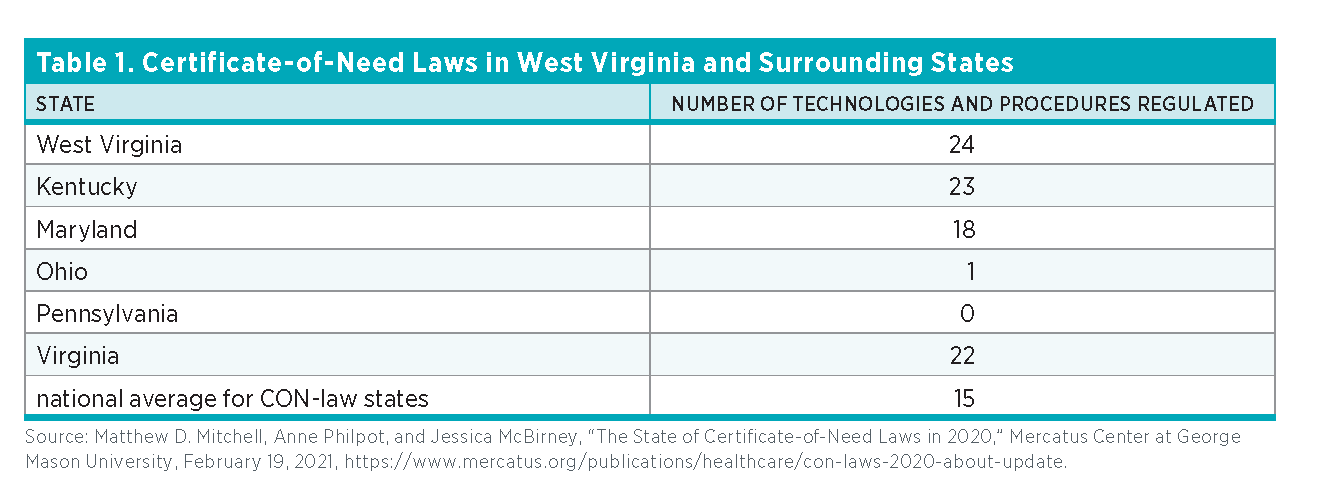
The state requires CONs for several services that are unlikely to be overprescribed, such as burn care, neonatal intensive care, renal failure treatment, and radiation therapy. The state also requires CONs for facilities and types of care that often go to vulnerable populations, such as substance abuse treatment, intermediate care facilities for those with intellectual disabilities, and psychiatric care. Some of the regulated services can be provided without expensive capital investments (home health and psychiatric care, for example). And some of these regulated services are lower-cost alternatives to hospital care such as hospice and ambulatory surgery. The following services and technologies are regulated under West Virginia’s CON program:
- Ambulatory surgical centers (ASCs)
- Cardiac catheterization
- Computed tomography (CT) scanners
- Home health
- Hospice
- Hospital beds
- Intermediate care facilities (ICFs) for individuals with intellectual disabilities
- Linear accelerator radiology
- Long-term acute care (LTAC)
- Magnetic-resonance imaging (MRI) scanners
- Mobile HI technology (CT/MRI/PET, etc.)
- Neonatal intensive care
- New hospitals or hospital-sized investments
- Nursing home beds/long-term care beds
- Obstetrics services
- Open-heart surgery
- Organ transplants
- Positron emission tomography (PET) scanners
- Psychiatric services
- Radiation therapy
- Rehabilitation
- Renal failure/dialysis
- Substance/drug abuse treatment
- Ultrasound
In addition, the state maintains a catch-all CON requiring providers to obtain a CON for any expenditure exceeding $5,618,381.
The Economics of CON Regulation
Unfortunately, by limiting supply and undermining competition, CON programs may undercut each of the laudable aims that policymakers desire to achieve with these rules. In fact, research shows that CON laws fail to achieve the goals most often given when enacting such laws. These goals include
- ensuring an adequate supply of healthcare resources,
- ensuring access to healthcare for rural communities,
- promoting high-quality healthcare,
- ensuring charity care for those unable to pay or for otherwise underserved communities,
- encouraging appropriate levels of hospital substitutes and healthcare alternatives, and
- restraining the cost of healthcare services.
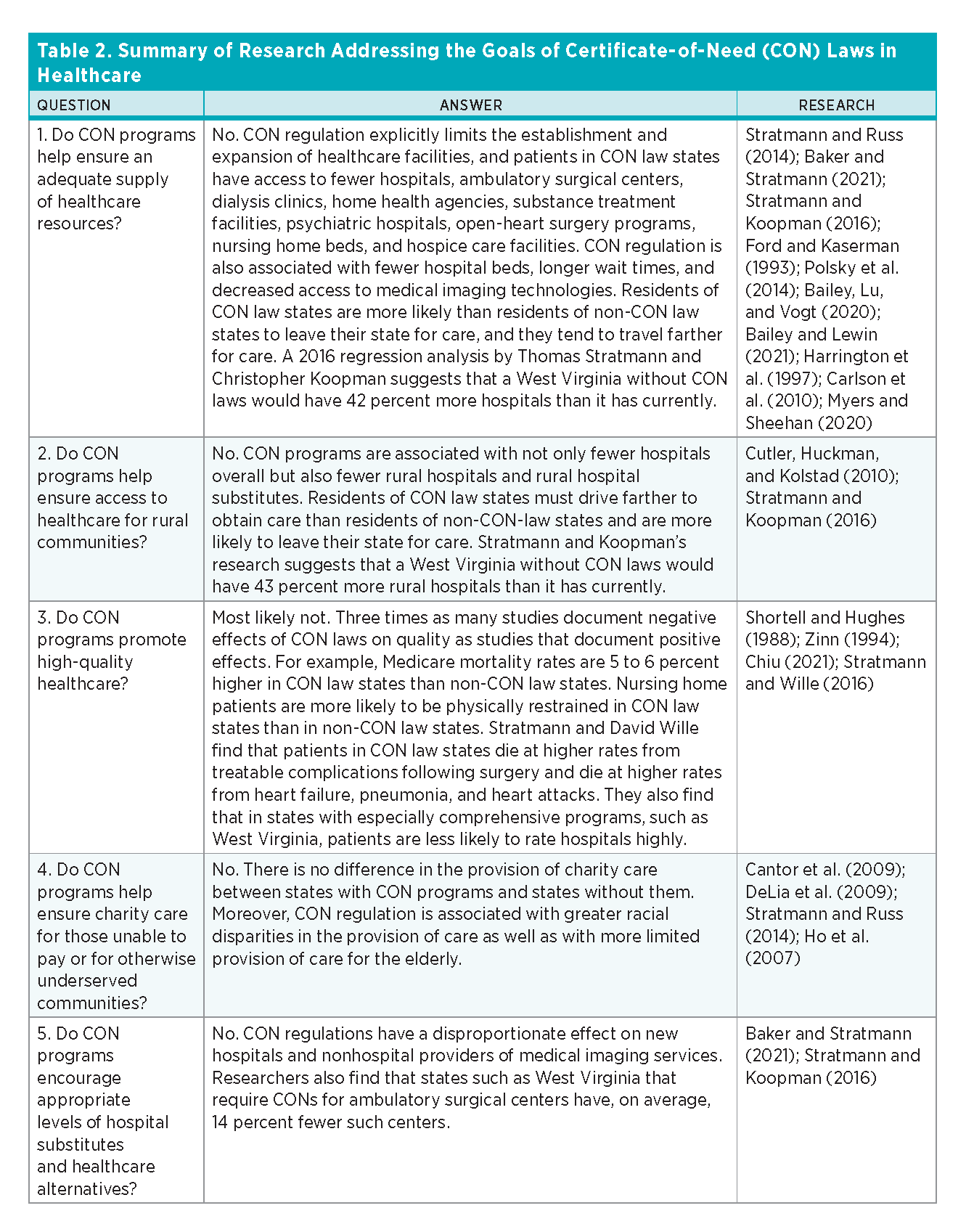
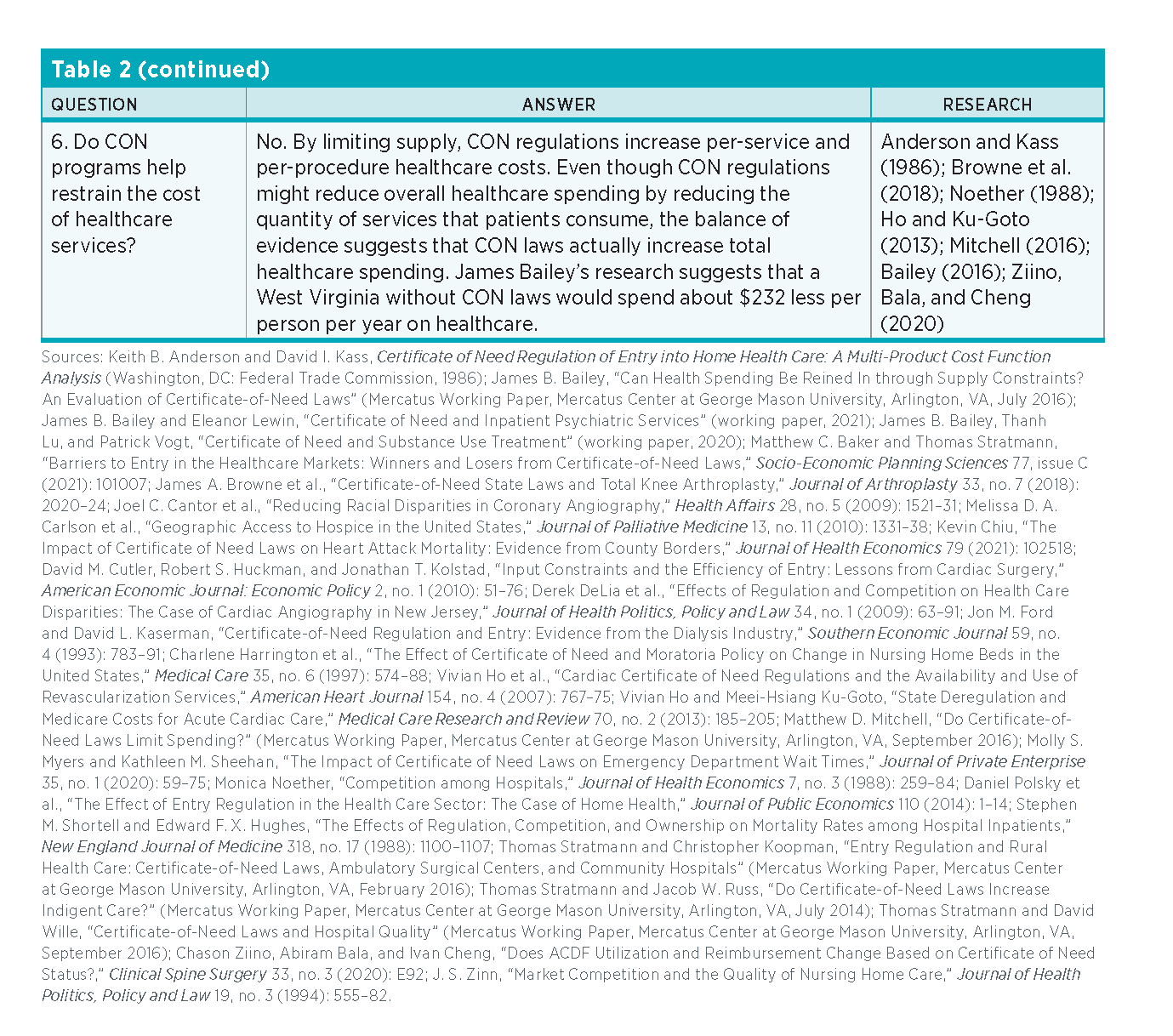
Researchers have ample information to help predict what would happen if West Virginia were to repeal its CON regulations because 15 states have repealed all or most of their CON requirements, and others have pared theirs back. Economists have used modern statistical methods to compare outcomes in CON and non-CON states to estimate the effects of these regulations. These methods control for factors such as socioeconomic conditions that might confound the estimates. Table 2 summarizes some of this research. It is organized around the stated goals of CON laws.
 Based on the experiences of other states, one can estimate what fiscal and health outcomes are likely to prevail in a West Virginia without CON regulation. These estimates are derived from cross-state regression analyses that track outcomes over decades. They account for socioeconomic differences as well as differences in the underlying health of the state populations.
Based on the experiences of other states, one can estimate what fiscal and health outcomes are likely to prevail in a West Virginia without CON regulation. These estimates are derived from cross-state regression analyses that track outcomes over decades. They account for socioeconomic differences as well as differences in the underlying health of the state populations.
Figure 1 shows the actual number of hospitals and ASCs as well as the estimated number of hospitals and ASCs in a West Virginia without CON regulation.
West Virginia’s rural hospitals are financially strained, so the effect of CON regulation on rural care is especially important to the state’s rural communities. Figure 2 shows the number of rural hospitals in West Virginia and estimates of how many there would be in a West Virginia without CON regulation.

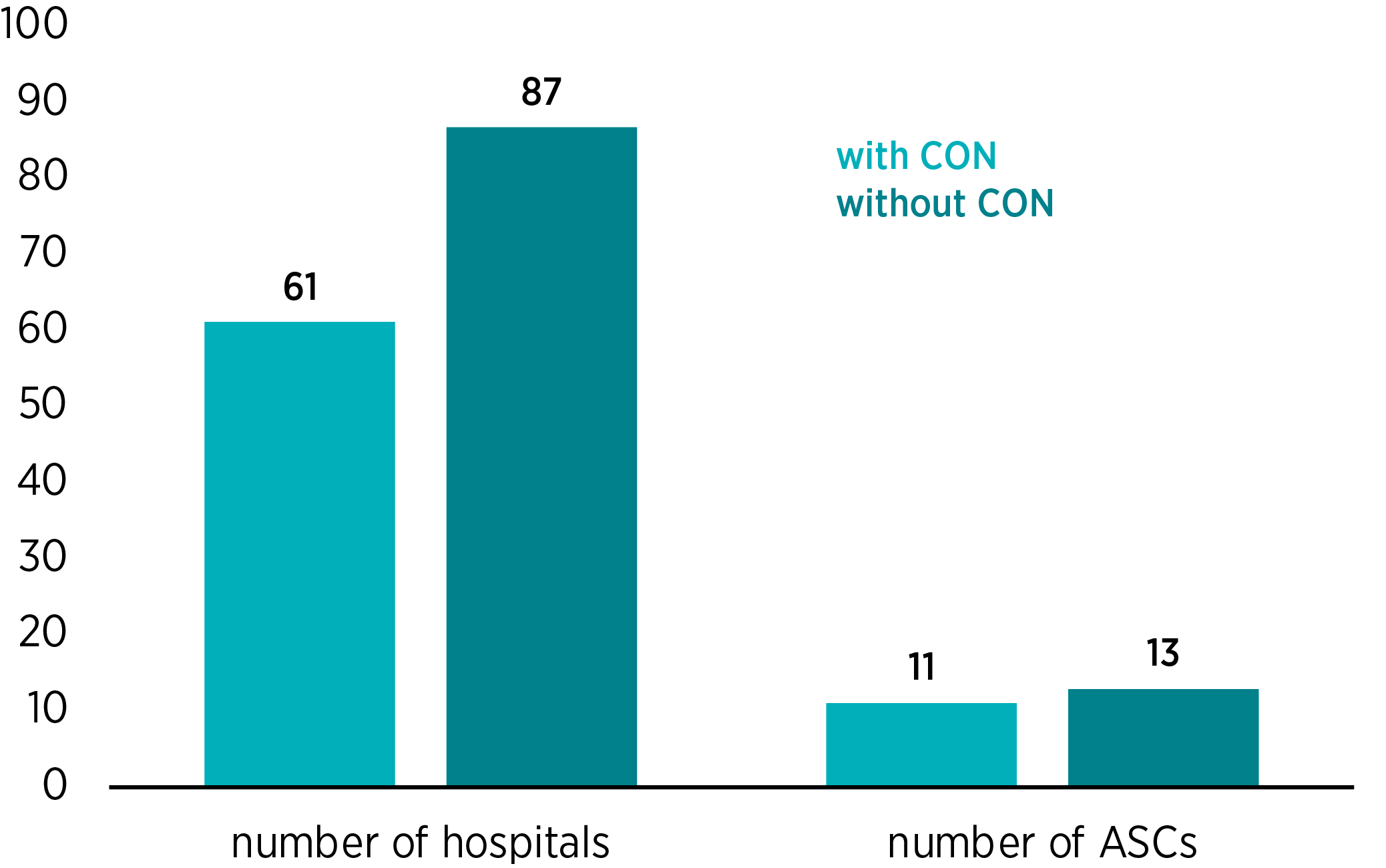

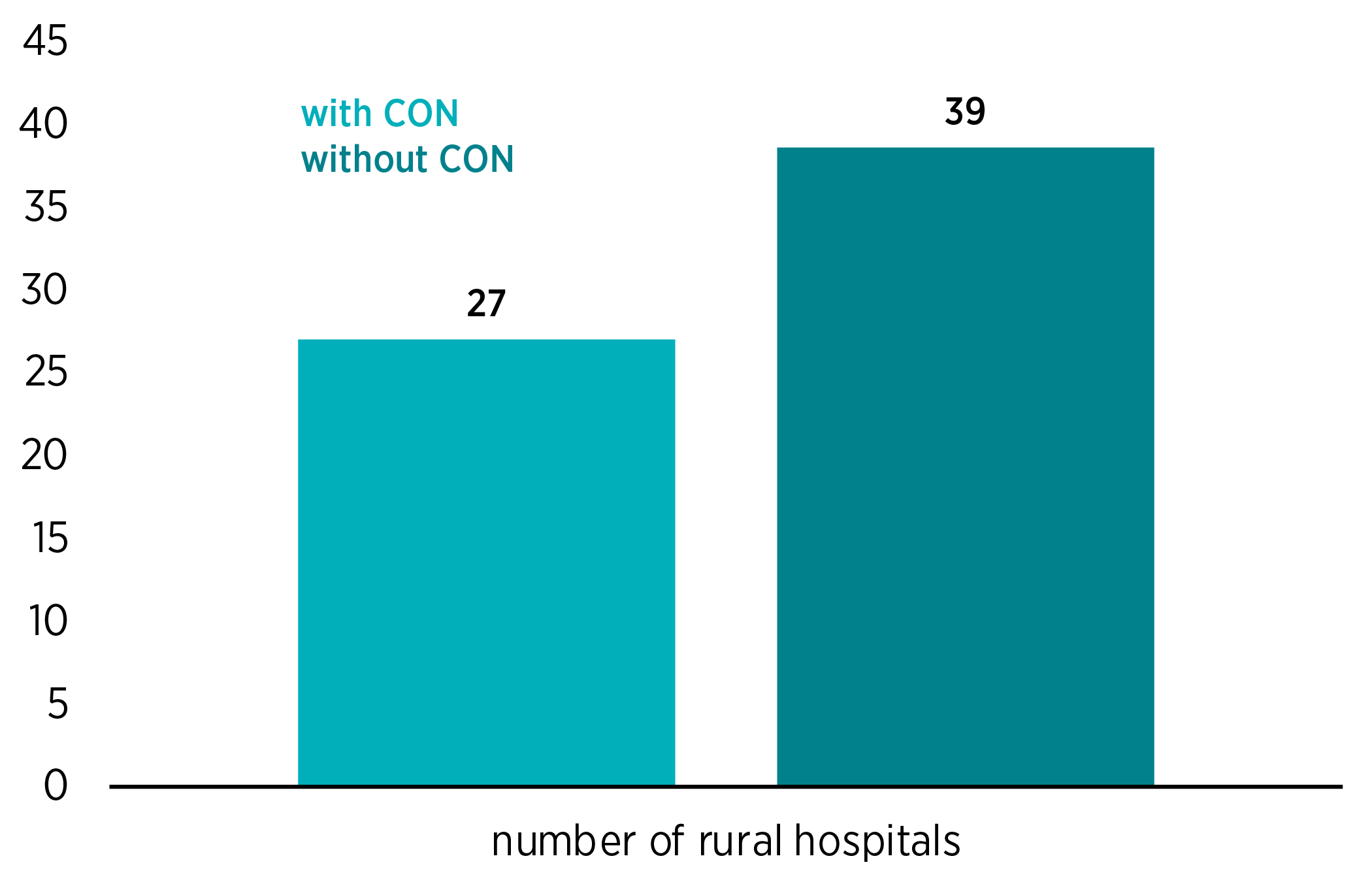
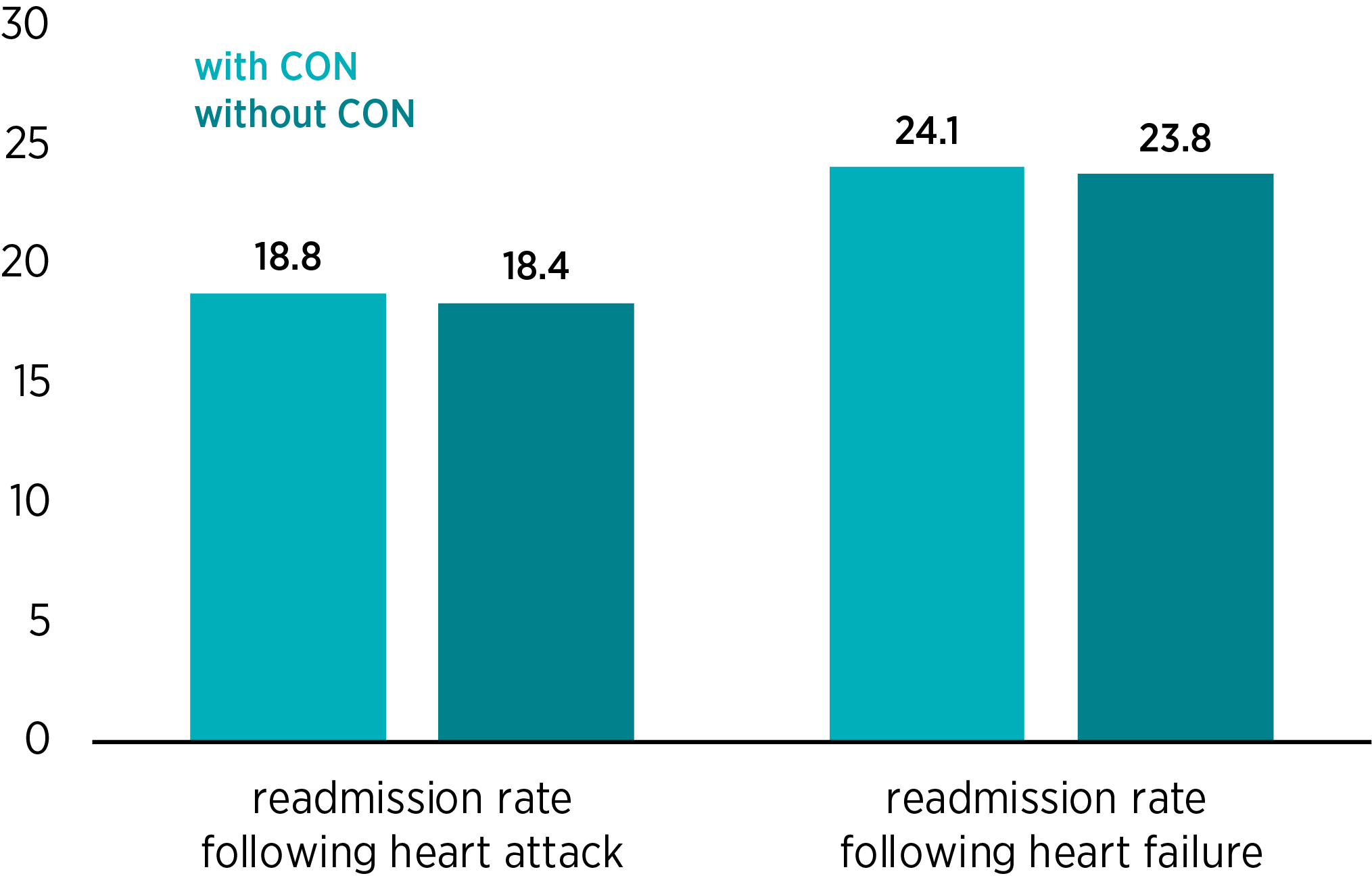
Figure 3 shows the actual and the estimated mortality rates following heart attack, heart failure, and pneumonia. Figure 4 shows the actual and estimated readmission rates following heart attack and heart failure.



In addition, researchers estimate that postsurgery complications would be approximately 5.5 percent lower and that the share of patients rating their hospital experience a 9 of 10 or 10 of 10 would be approximately 4.9 percent higher in a West Virginia without CON regulation. Finally, economists estimate that annual per capita healthcare spending would be approximately $232 lower in a West Virginia without CON regulation.
Reform Options
The weight of evidence suggests that a full repeal of CON laws would expand access to healthcare in West Virginia that is of both high quality and low cost. Repeal might be scheduled to take effect in the near future or at a later date. Alternatively, policymakers might phase in repeal by requiring the CON board to approve an ever-larger percentage of applications over a certain number of years.
Short of full repeal, policymakers have several options to reform the program and limit its negative effects. For example, the state might eliminate specific CON requirements. Some requirements ripe for reform include
- CONs that restrict access to facilities and services used by vulnerable populations, such as substance abuse treatment, intermediate care facilities for those with intellectual disabilities, or psychiatric services;
- CONs for services that are unlikely to be overprescribed, such as neonatal intensive care, renal failure treatment, and radiation therapy;
- CONs for services that require limited capital expenditures, such as psychiatric services or home health; and
- CONs that restrict access to low-cost modes of care, such as hospice and ASCs.
Policymakers might also consider a number of options to ease the administrative burden of CON laws. For example, they might reduce West Virginia’s fees, reduce the administrative burden of the application process, or require incumbents who unsuccessfully challenge an entrant’s CON application to pay the entrant’s legal and compliance costs. Going further, the state could follow Indiana, Louisiana, Michigan, Nebraska, and New York and no longer solicit or consider the objections of a competitor when a provider applies for a CON, given that the process is manifestly anticompetitive.
The criteria used to evaluate a CON application might also be changed. For example, a CON application should not be rejected to prevent the provision of duplicative services. Such a rejection guarantees monopoly status for the current service provider in the area, and healthcare monopolies are associated with high-cost and low-quality care. Utilization rate is another poor criterion. If an existing hospital knows that potential competitors are less likely to obtain CONs if it keeps its bed utilization rate low, then it faces an incentive to acquire more beds than it needs and ensure that many of them remain empty. This is exactly the sort of unnecessary capital expenditure that CON regulation was supposed to discourage.
In addition, the state might raise the $5.6 million monetary threshold for investments that necessitate a CON. It might bar those with a financial interest in incumbent providers from serving on the board of the West Virginia Health Care Authority. It might also require the board to seek input from parties without financial interest in the outcome or from parties dedicated to the preservation of market competition and patient outcomes, such as patient health advocates, economists, or antitrust authorities at the FTC.
Finally, policymakers might consider a number of options that would increase the transparency of the CON program and make legislative oversight easier. One option would be to require the board to regularly disclose the CON approval rate. The regulator could also be required to report the share of applications opposed by incumbent providers as well as the different approval rates for opposed and unopposed applications.
The regulator could also be required to ask applicants to estimate their costs of applying for a CON and then regularly report these numbers to the public. And finally, the regulator could be required to follow up with denied applicants to evaluate how the denial has affected their provision of services.
Conclusion
Given the substantial evidence that CON regulations do not achieve their stated goals, one may wonder why these rules continue to exist in so much of the country. The explanation seems to lie in the special-interest theory of regulation. Specifically, CON regulations perform a valuable function for incumbent providers of healthcare services by limiting their exposure to new competition. Researchers find greater market concentration in CON law states than in non-CON law states. Moreover, the average provider in a CON law state has a significantly higher volume of patients. Provider profits fall in states that remove CON laws (though profits recover after a few years). These facts, combined with the fierce opposition to deregulation by industry insiders, suggest that the rules do indeed protect incumbents’ profits. Furthermore, political donations have been shown to increase the odds that a CON request will be granted, so the rules may invite corrupt quid pro quos.
Whereas patients and payers are harmed by the regulation, hospital executives benefit from it. Researchers find that urban hospital CEO pay is over $90,000 higher in CON law states than in non-CON law states.
These aspects of CON regulation are why economists as well as antitrust authorities have long believed that these regulations are anticompetitive and harmful to consumers.

