Certificate-of-need (CON) laws require healthcare providers to seek permission from state regulators before they offer new services, expand facilities, or invest in technology. Researchers find that these laws tend to restrict access to healthcare, make services more expensive, and undermine the quality of care.
Over the past decade, there have been a number of attempts to quantify state CON regulation. The most notable of these include research from the American Health Planning Association in 2016, the National Conference of State Legislatures in 2019, and the Institute for Justice in 2020. We add to these efforts and improve on our own past research by providing a single, comprehensive source that shows the current status of CON regulation in all 50 states and the District of Columbia.
The History of CON Laws
Nearly six decades ago, New York became the first state to enact a CON law for healthcare services. A decade later, the federal government mandated state implementation of CON regulation in an effort to control healthcare costs, increase access to care, and improve quality. When early research suggested that CON regulations were failing to meet these goals, the federal government repealed the mandate, but many states kept their CON programs on the books.
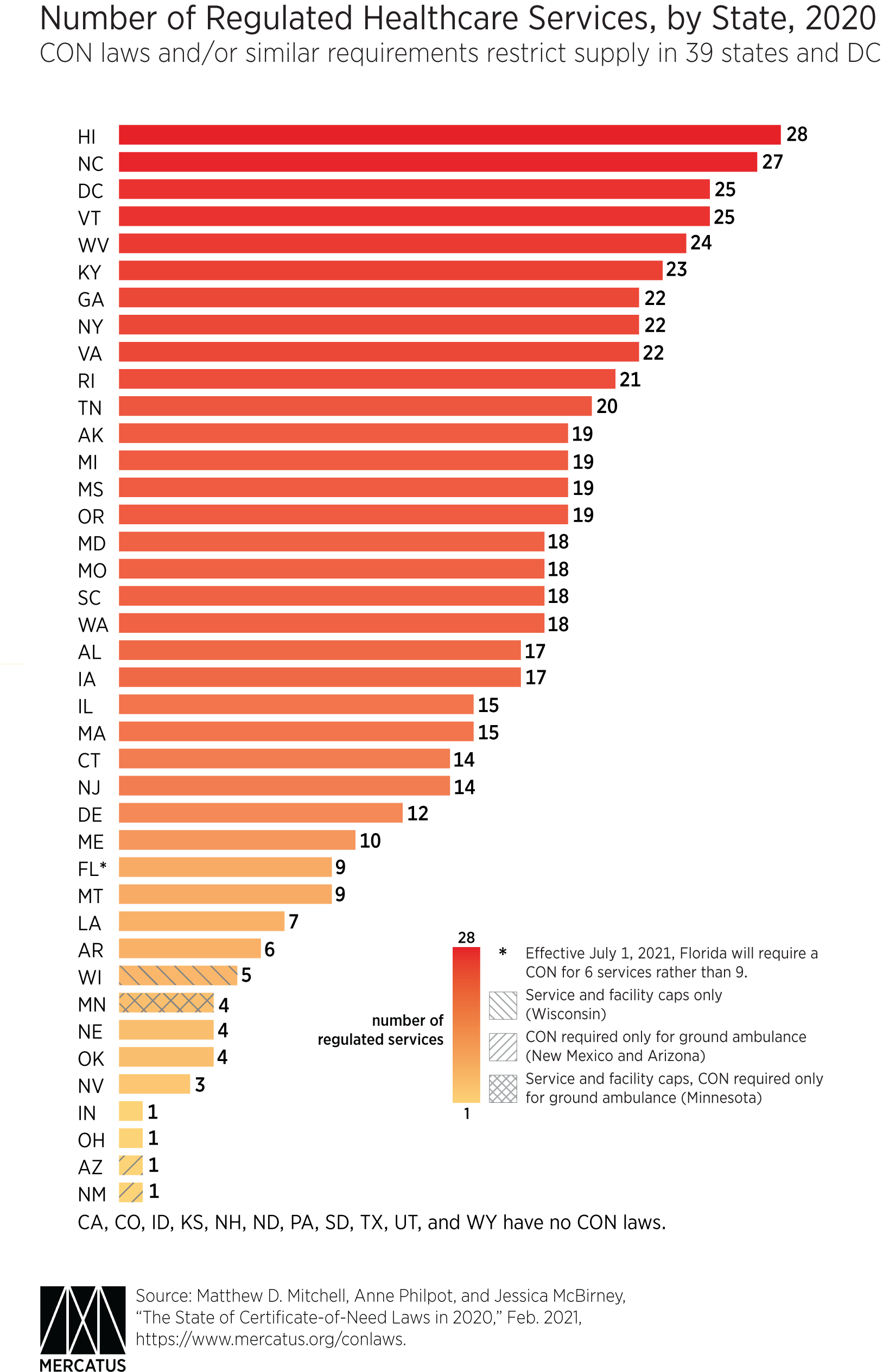
As of January 2020, 35 states and the District of Columbia required providers to obtain a CON before offering at least one healthcare service. Two additional states, Minnesota and Wisconsin, set numerical caps on certain services such as the total number of hospital beds and nursing home beds. Other states require a CON for ground and air ambulance services, though these laws are often found in transportation statutes, and their effects on health outcomes are not as well studied. If one includes states with caps as well as those that require a CON for ambulance services, then the total number of states with CON or CON-like regulations of healthcare services rises to 39, plus the District of Columbia (see the accompanying chart).
What’s New in the Latest Version?
Since the previous edition of this project, we have added three important categories: (1) CON regulations for new hospital construction or hospital-sized capital investments, (2) caps on services and facilities, and (3) ambulance CON regulations, even in otherwise non-CON states.
Our Findings
Across 35 regulated services, we find that the most common CON requirements are for nursing homes, psychiatric services, and hospitals (new construction and expansion). Regulating 28 services, Hawaii has the highest number of CON requirements of any state. North Carolina (27 services) and the District of Columbia (25 services) fall close behind. Meanwhile, Indiana and Ohio each regulate one service, and Arizona and New Mexico have only ambulance service CON requirements. Wisconsin has caps on services and facilities, but no statewide CON requirement. Minnesota has ambulance CON requirements and caps on services and facilities. Eleven states have no CON laws or caps: California, Colorado, Idaho, Kansas, New Hampshire, North Dakota, Pennsylvania, South Dakota, Texas, Utah, and Wyoming (see the accompanying chart).
Our Methods
Our latest data are drawn from each state’s statutes, regulations, and agency documents. Where these sources were contradictory or ambiguous, we relied on direct communication with administrators.
The following principles guided our research:
- If any portion of a category of healthcare service requires CON approval, we consider this a regulated category for our purposes. For example, if a state’s CON requirement for MRI machines applies only to certain independent facilities, we count the whole category of MRI machines as CON regulated in that state—even though the MRI CON requirement is not universally applicable to all providers.
- Except for the “hospital-sized investments” category, we do not automatically count services and equipment on the basis of CON-cost thresholds alone. Some states impose a low-cost threshold. But because we do not attempt to estimate the costs associated with any category, we do not categorize a service as being regulated unless it is explicitly mentioned in the law.
- Whereas our analysis covers only state CON laws, some local governments have additional CON requirements in their jurisdictions. These local CON laws are not represented in the statewide data. However, if a state requires its local governments to establish and enforce a particular CON requirement at the local level, we count this toward the state’s total.
Moving Forward
Some states, such as Florida, have taken steps to repeal or otherwise reform their CON laws. Some of the changes adopted by Florida will take effect in mid-2021, reducing the number of regulated services in the state from 9 to 6. But more than two-thirds of the states continue to restrict entry, expansion, and competition in healthcare through CON laws. There is still more to be done to achieve greater access to low-cost, high-quality healthcare.

