- | Corporate Welfare Corporate Welfare
- | Data Visualizations Data Visualizations
- |
40 Years of Certificate-of-Need Laws Across America
Forty years of peer-reviewed academic research—including the latest studies by researchers at the Mercatus Center at George Mason University—suggests that CON laws have not only failed to achieve their goals but have in many cases led to the opposite of what those who enacted the laws intended.
In the summer of 2016, New Hampshire became the 15th state to repeal its “certificate-of-need” (CON) program. This means that 35 states and the District of Columbia currently prohibit entry or expansion of healthcare facilities through CON programs. These laws, which require government permission before a facility can expand, offer a new service, or purchase certain pieces of equipment, were enacted in the belief that they would achieve several goals.
- Ensure an adequate supply of health resources
- Ensure rural community access to care
- Increase the quality of care
- Ensure the provision of charity care to those unable to pay and for other underserved communities
- Encourage the use of hospital substitutes such as ambulatory surgery center (ASCs)
- Restrain the cost of care
Consider, for example, the stated aim of CON laws of increasing the supply of healthcare services. GMU professor and Mercatus Center scholar Thomas Stratmann and his coauthor Jake Russ found that CON is associated with a more limited supply of hospital beds and medical imaging equipment. In related research, Stratmann and PhD student Matthew C. Baker found that CON is associated with less utilization of medical imaging equipment among nonhospital providers.
Or consider the goal of increasing rural access to care. Stratmann and Mercatus Center research fellow Christopher Koopman found that CON is associated with fewer, not more, rural hospitals.
Though policymakers didn’t originally intend CON as a quality-enhancing regulation, many advocates now contend that it might increase quality by channeling more procedures through fewer hospitals, allowing those hospitals to gain expertise. In research with Mercatus MA fellow David Wille, however, Professor Stratmann finds that CON regulation is associated with lower, not higher, quality, as measured along multiple dimensions.
The now-repealed federal statute that encouraged states to adopt CON laws explicitly stated that one goal of CONs was to encourage the appropriate use of hospital substitutes such as ambulatory surgery centers (ACSs). Ironically, however, 28 states currently require ASC-specific CONs, effectively limiting the supply of these hospital substitutes. Some CON advocates defend these limits by contending that these lower-cost centers take the highest-paying customers away from hospitals. But Stratmann and Koopman’s work found that CON regulations seem to limit the supply of both ASCs and traditional hospitals.
Nor does the evidence suggest that these regulations advance the goal of reducing healthcare costs. On the contrary, the preponderance of evidence suggests that these regulations are associated with higher healthcare prices and higher overall healthcare spending, as is evident in Matthew Mitchell’s review of decades of research as well as in the latest research by Professor James Bailey of Creighton University.
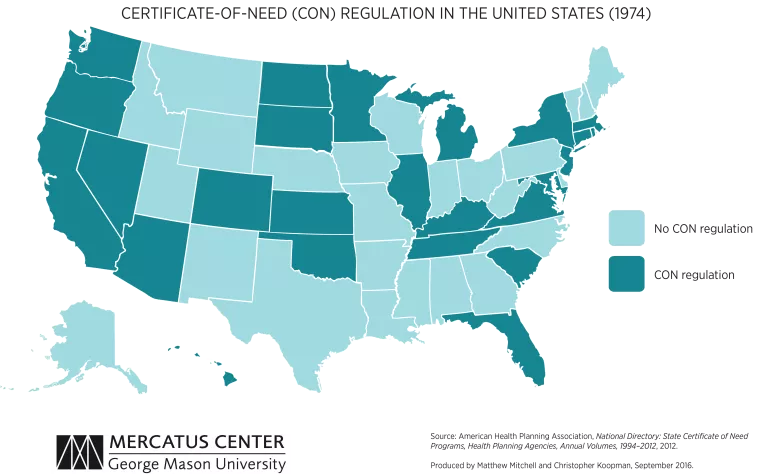
As these maps show, the first state to institute a CON program was New York in 1964, followed by Rhode Island, Maryland, California, and 22 other states over the next 10 years. In 1974, Congress passed the National Health Planning and Resources Development Act, requiring states to implement CON requirements in order to receive funding through certain federal programs. Louisiana was the only state not to implement a CON program during this time.
In 1986, the federal government repealed the CON mandate, and many states immediately began retiring their CON programs. By 1990, California, Colorado, Idaho, Kansas, Minnesota, New Mexico, South Dakota, Texas, Utah, Wisconsin, and Wyoming (a total of 11 states) had repealed their CON programs. (Arizona dropped CON regulations for most procedures but continued a regulation that limits air ambulances. Because of its limited scope, most analysts exclude Arizona from their empirical studies. For the purposes of this map, however, we include it as a CON state.) This left 39 states and the District of Columbia with these laws, although Wisconsin reinstated its program in 1993.
By 2000, Indiana, North Dakota, and Pennsylvania had repealed their programs. This brought the number of states with CON programs to 37 (and DC). Since 2000, Wisconsin had been the only state to repeal its CON program until New Hampshire did so in 2016. So now 35 states and the District of Columbia retain these restrictions.

