- | Healthcare Healthcare
- | Research Papers Research Papers
- |
Healthcare Openness and Access Project 2020: Full Release
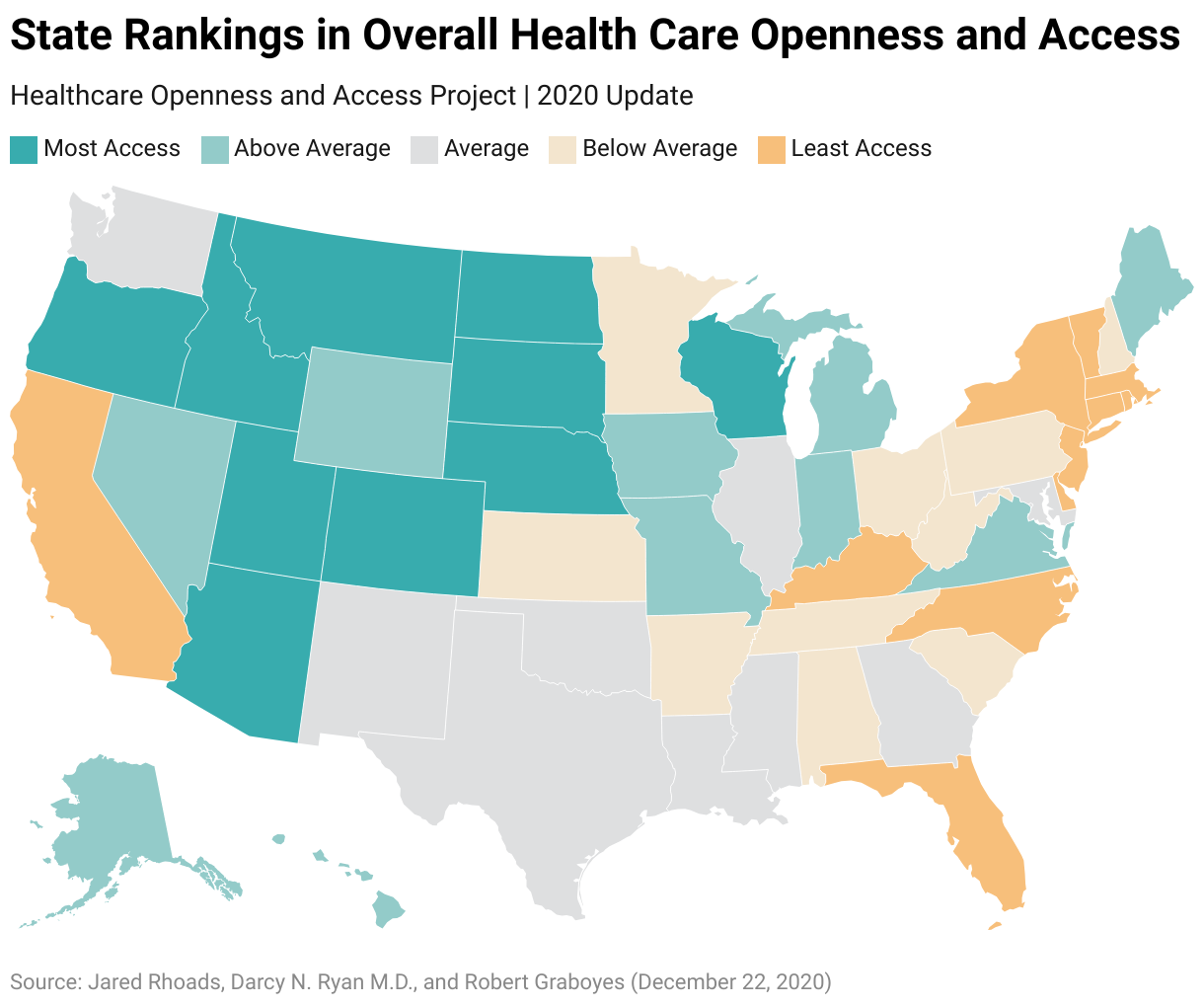
State-by-state measures of the flexibility and discretion that patients and providers have in managing health and healthcare
There is broad agreement about the desirability of lowering the cost and improving the quality of US healthcare and of broadening health insurance coverage. States have (and should have) substantial control over healthcare delivery—and not solely or principally in the area of insurance reform. To make the best use of state powers in improving care, it is vital to compare how healthcare institutions work across the states. In “Healthcare Openness and Access Project 2020: Full Release,” Jared M. Rhoads, Darcy N. Bryan, and Robert F. Graboyes present state-by-state measures of the flexibility and discretion that patients and providers have in managing health and healthcare.
The Healthcare Openness and Access Project (HOAP) seeks to raise important questions, such as how open each state’s laws and regulations are to institutional variation in the delivery of care and how much access to varying modes of care this openness confers on the state’s patients and providers. The goal of HOAP is to encourage these types of questions rather than to provide definitive answers.
NOTE: A preliminary version of this report was rush-released in the spring of 2020 to help policymakers cope with the unfolding COVID-19 pandemic. This new version incorporates small changes, clarifications, and peer-review feedback that we have collected since that time. We note that the data in this document mostly reflect the status quo ante prevailing just as the pandemic began. Over the course of 2020, most states have somewhat relaxed regulations for the duration of the public health emergency. Were we to incorporate these temporary changes into our data, it is likely that most states’ scores would rise. Thus, future HOAP scores may be greatly impacted by whether state regulations return to the early-2020 status quo or whether these emergency measures become permanent.
Background and Study Design
HOAP’s overall index averages five equally weighted categories of indicators (variables) that measure the discretion of patients, providers, and institutions over broad areas of healthcare, such as public health and telemedicine. The equal weighting of indicators within each category is an explicit recognition of the fact that no single set of weights should be considered “correct.” HOAP is constructed so that readers and researchers can alter the weights assigned to different variables to reflect their own preferences.
The first iteration of HOAP (HOAP 2016) was issued in December 2016. HOAP 2018, issued in June of that year, revised the data to reflect changes in state laws in the interim and to reflect modest changes in sources of data. HOAP 2020 incorporates new indicators that may better represent the discretion states allow in the provision of healthcare goods and services.
HOAP 2020’s five categories replace the previous editions’ 10 subindexes. Changes in state rankings between 2018 and 2020 reflect both changes in methodology and changes in states’ laws and regulations, so one should be cautious about reading too much into the numeric differences between HOAP 2018 and HOAP 2020.
Key Takeaways
- Insurance isn’t the only issue. To be sure, insurance is a very important part of the healthcare system, and HOAP does include some insurance-related indicators. However, simultaneous progress on the three goals of healthcare reform (lower costs, higher quality, and broader coverage) will require fundamental changes in the technologies and structures of care and in how, where, when, and why care is delivered. HOAP highlights institutional features that help determine the degree to which experimentation is possible.
- States matter in healthcare policy. States possess great power to determine which providers may perform what services, the means by which they may do so, their legal responsibilities in the event that patients suffer harm, and so forth. The HOAP index suggests how the states differ in encouraging delivery-system innovation.
- Perception of state policies does not always match reality. For example, a leftward tilt in the Affordable Care Act debate does not necessarily correlate with tight centralized control of healthcare at the state level. Nor does a rightward tilt in the debate always comport with extensive patient-provider discretion. For example, HOAP data suggest that “blue” states Oregon and Hawaii offer broad leeway to patients and providers, while “red” states Arkansas and Kentucky have some of the most restrictive healthcare laws and regulations in the nation.
- Comparisons among states are important. HOAP as a whole provides a great deal of comparative data on healthcare policy in the states. It is a one-stop source of information on policy differences around the country. As an example, 41 states require a physician’s signature to prescribe oral contraceptives. So, to many, that requirement may seem to be the natural order of things, a universal. But 10 jurisdictions (including the District of Columbia) allow pharmacists to autonomously prescribe oral contraceptives. Perhaps this anomaly will persuade policymakers in other states to at least ask how that market functions in those 10 jurisdictions.
- Discussion is valuable for determining how to move forward. HOAP should become a catalyst for discussion, but it is not the definitive measure of openness, access, flexibility, or discretion in healthcare for any particular state. If observers question aspects of the index and offer alternative measures, then the project will have done its job.
Related Content
- | Academic & Student Programs Academic & Student Programs
- | Healthcare Healthcare
- | Research Papers Research Papers
2018 Edition: Healthcare Openness and Access Project

- | Healthcare Healthcare
- | Mercatus Original Video Mercatus Original Video
What Is the Healthcare Openness and Access Project?

- | Healthcare Healthcare
- | Research Papers Research Papers

